ACUERDO por el que se emiten las Reglas de Operación del Programa de Abasto Social de Leche, a cargo de Liconsa, S.A. de C.V. (LICONSA), para el ejercicio fiscal 2020.
Al margen un sello con el Escudo Nacional, que dice: Estados Unidos Mexicanos.- AGRICULTURA.- Secretaría de Agricultura y Desarrollo Rural.
VICTOR MANUEL VILLALOBOS ARÁMBULA, Secretario de Agricultura y Desarrollo Rural, con fundamento en los artículos 4, párrafo tercero, 25 y 26 apartado A, 27, fracción XX y 28, párrafo decimotercero de la Constitución Política de los Estados Unidos Mexicanos; 9, 12, 23, 26, 35 y Artículo Décimo Séptimo Transitorio de las modificaciones publicadas en el Diario Oficial de la Federación el 30 noviembre de 2018, de la Ley Orgánica de la Administración Pública Federal; 4 de la Ley Federal de Procedimiento Administrativo; 9, 12, 33, 34, 35 y 40 de la Ley de Planeación; 75 y 77 de la Ley Federal de Presupuesto y Responsabilidad Hacendaria y 176 de su Reglamento; 1, 72, 140, 178, 179, 180, 183 y 189 de la Ley de Desarrollo Rural Sustentable; 1 y 70 fracciones I, XV, XIX, XX, XXVI y XXVIII de la Ley General de Transparencia y Acceso a la Información Pública; fracción XII, 26, 27 y 32, los Anexos 11, 25 y 26, y los Artículos Tercero, Quinto y Décimo Tercero Transitorios del Decreto de Presupuesto de Egresos de la Federación para el Ejercicio Fiscal 2019; y 1, 3 y 5, fracción XXII del Reglamento Interior de la Secretaría de Agricultura, Ganadería, Desarrollo Rural, Pesca y Alimentación; y
CONSIDERANDO
Que la Constitución Política de los Estados Unidos Mexicanos, establece en su Artículo 25 que corresponde al Estado la rectoría del desarrollo nacional para garantizar que sea integral y sustentable, que fortalezca la Soberanía de la Nación y su régimen democrático y que, mediante el fomento del crecimiento económico y el empleo, así como una más justa distribución del ingreso y la riqueza, permita el pleno ejercicio de la libertad y la dignidad de los individuos, grupos y clases sociales;
Que la Ley Federal de Presupuesto y Responsabilidad Hacendaria dispone que la Cámara de Diputados en el Presupuesto de Egresos, podrá señalar los programas, a través de los cuales se otorguen subsidios, que deberán sujetarse a reglas de operación con el objeto de asegurar que la aplicación de los recursos públicos se realice con eficiencia, eficacia, economía, honradez y transparencia. Asimismo, se señalarán en el Presupuesto de egresos los criterios generales a los cuales se sujetarán las reglas de operación de los programas;
Los resultados de la Encuesta Nacional de Salud y Nutrición (Ensanut) 2012, resalta que 13.6 por ciento de las y los niños mexicanos menores de cinco años, padecen desnutrición crónica y en las zonas rurales del país se eleva hasta el 27.4 por ciento.
Que los programas de subsidios del Ramo Administrativo 08, "Agricultura y Desarrollo Rural", entre ellos el Programa de Abasto Social de Leche a cargo de Liconsa, S.A. de C.V. (LICONSA), se destinarán, en las entidades federativas, en los términos de las disposiciones aplicables, exclusivamente a la población en condiciones de pobreza, de vulnerabilidad, de adultos mayores, de rezago y de marginación, de acuerdo con los criterios de resultados que defina el Consejo Nacional de Población y la Declaratoria de Zonas de Atención Prioritaria formulada por la Cámara de Diputados, mediante acciones que promuevan la superación de la pobreza a través de la educación, la salud, la alimentación nutritiva y de calidad, la generación de empleo e ingreso, autoempleo y capacitación; protección social y programas asistenciales; y el fomento del sector social de la economía;
Que para contribuir a las Directrices del Plan Nacional de Desarrollo 2019-2024, este Programa se encuentra alineado a la Directriz 3 "Desarrollo Económico Incluyente";
Que el Artículo 77 de la Ley Federal de Presupuesto y Responsabilidad Hacendaria ordena que las Reglas de Operación deberán ser simples y precisas, con el objeto de facilitar la eficiencia y la eficacia en la aplicación de los programas;
Las presentes Reglas de Operación no se contraponen, afectan o se duplican con otros Programas y/o acciones del Gobierno Federal, en cuanto a su diseño, beneficios, apoyos otorgados y población objetivo. Lo anterior de conformidad con lo dispuesto en el artículo 179 del Realimento de Ley Federal de Presupuesto y Responsabilidad Hacendaria;
Que para asegurar la coordinación de acciones entre dependencias y entidades y evitar duplicidad en el ejercicio de los recursos y reducir gastos administrativos este Programa se apega a lo dispuesto en el artículo 75 fracción VII de la Ley Federal de Presupuesto y Responsabilidad Hacendaria; y
Que para cumplir con todo lo anterior, en todo caso se cuidará aplicar las leyes y demás normas en vigor en lo que toca a la igualdad de derechos entre hombres y mujeres, la eliminación de toda forma de discriminación y se buscará en todas las acciones, tener presentes los principios de sustentabilidad para preservar y mejorar el medio ambiente.
En este tenor, he tenido a bien emitir el siguiente:
ACUERDO POR EL QUE SE EMITEN LAS REGLAS DE OPERACIÓN DEL PROGRAMA DE ABASTO
SOCIAL DE LECHE, A CARGO DE LICONSA, S.A. DE C.V. (LICONSA), PARA EL EJERCICIO FISCAL
2020.
SOCIAL DE LECHE, A CARGO DE LICONSA, S.A. DE C.V. (LICONSA), PARA EL EJERCICIO FISCAL
2020.
GLOSARIO DE TÉRMINOS
Para efectos y aplicación del Programa y sus Componentes, en las presentes Reglas de Operación independientemente de que el término se utilice en plural o singular, se entenderá por:
Actor Social y Comunitarios.- Es una agrupación de personas con un fin determinado, legalmente constituidas bajo la figura jurídica de persona moral, con objeto social y/o comunitario sin fines de lucro.
Comité de Beneficiarios.- Es una agrupación social de interés comunitario sin personalidad jurídica ni relación laboral con Liconsa que apoya la operación del punto de venta para que se realice en forma ordenada y de acuerdo a la normatividad establecida.
Convenios con Actores Sociales y Comunitarios.- Son aquellos celebrados con instituciones públicas de los tres órdenes de gobierno: federal, estatal y municipal, con aquellas instituciones de asistencia pública, personas morales legalmente constituidas, así como organizaciones comunitarias indígenas y de vecinos, todos sin fines de lucro.
Convenio Modificatorio.- Son aquellos que se celebran con los actores sociales y comunitarios, a fin de modificar lo pactado en el convenio principal suscrito con Liconsa, para ajustar el número de personas beneficiarias, el suministro por día autorizado y/o la persona representante legal, entre otros términos.
Cuestionario Único de Actores Sociales y Comunitarios.- Instrumento de recolección de información en el que se registran los actores sociales que reciben apoyos.
Información Socioeconómica.- Instrumento de recolección de información en el que se captan los datos sobre las condiciones socioeconómicas y demográficas del hogar y sus integrantes para la identificación de los posibles beneficiarios.
Estudio de factibilidad.- Formato para recopilar datos relevantes acerca de la cantidad potencial de personas beneficiarias, la disponibilidad de local, la ubicación de la zona en donde se requiere instalar un nuevo punto de venta, etc., que sirve para dictaminar la procedencia o no de su instalación. Se puede consultar en el Manual de Procedimiento para la Apertura, Reubicación y Cierre de Lecherías, el cual se encuentra la página electrónica www.gob.mx/liconsa.
Ficha socioeconómica.- Cuestionario que se aplica a los Actores Sociales y Comunitarios, mediante la cual se determina la factibilidad de incorporarse al Programa de Abasto Social de Leche.
Hogar.- Es un conjunto de personas que hacen vida en común dentro de una misma vivienda, unidos o no por parentesco y que comparten los gastos de manutención y preparan los alimentos en la misma cocina.
Vivienda.- Espacio fijo delimitado generalmente por paredes y techos de cualquier material, con entrada independiente que se construyó o adaptó para el alojamiento de personas. XI. Jefe (a) de hogar.- Persona que forma parte del hogar, que toma las decisiones importantes y a quien se le reconoce de forma natural como el líder por parte de los demás integrantes por su edad, experiencia, autoridad, respeto o por razones de dependencia
Leche fortificada.- Leche líquida o en polvo que distribuye Liconsa, y que, adicionalmente a su contenido de proteínas, grasa, lactosa, minerales y vitaminas A y D, contiene cantidades importantes de vitaminas B2, B12, ácido fólico, hierro y zinc.
Padrón de beneficiarios.- Relación oficial de beneficiarios que incluye a las personas atendidas por los
programas federales de Desarrollo Social cuyo perfil socioeconómico se establece en la normatividad correspondiente.
Personas Beneficiarias.- Aquellas personas que forman parte de la población atendida por los programas de desarrollo social que cumplen los requisitos de la normatividad correspondiente.
Perspectiva de Género.- Se refiere a la metodología y los mecanismos que permiten identificar, cuestionar y valorar la discriminación, desigualdad y exclusión de las mujeres, que se pretende justificar con base en las diferencias biológicas entre mujeres y hombres, así como las acciones que deben emprenderse para actuar sobre los factores de género y crear las condiciones de cambio que permitan avanzar en la construcción de la igualdad de género.
Personal de Promotoría Social.- Es la persona responsable de la administración del padrón de beneficiarios y el enlace con el público en general en los puntos de venta
Punto de venta.- Es el lugar al cual acuden las personas beneficiarias a recoger su dotación de leche.
Unidades operativas.- Lugar o lugares donde los actores sociales y comunitarios entregan la leche a sus beneficiarios.
Tarjeta de dotación de leche.- Instrumento oficial que identifica a la persona titular y que indica la cantidad de leche que puede retirar, de acuerdo con el número de personas beneficiarias registradas en el padrón.
Titular de la tarjeta de dotación. Es la persona que representa al hogar inscrito en el Programa, identificada para recibir la dotación de leche y realizar cualquier trámite relacionado al mismo.-
Localidad.- De acuerdo con el Marco Geoestadístico es el lugar ocupado con una o más edificaciones utilizadas como viviendas, las cuales pueden estar habitadas o no, este lugar es reconocido por un nombre dado por alguna disposición legal o la costumbre.
Matriz de Indicadores para Resultados (MIR).- Es una herramienta de planeación que en forma resumida, sencilla y armónica establece con claridad los objetivos de un programa, incorpora los indicadores que miden dichos objetivos y sus resultados esperados. También identifica los medios para obtener y verificar la información de los indicadores e incluye los riesgos y contingencias que pueden afectar el desempeño del programa.
CONTENIDO
TITULO PRIMERO. Disposiciones Generales
Capítulo I Lineamientos cardinales
Artículo Primero Establecimiento de las Reglas de Operación de Liconsa, S.A. de C.V.
Artículo Segundo Objetivo General del Programa.
Artículo Tercero Objetivo Específico.
Artículo Cuarto Población Objetivo.
Artículo Quinto Cobertura.
Artículo Sexto Requisitos Generales para el Otorgamiento de los Incentivos.
Artículo Séptimo Tipos y Montos de Apoyo.
TITULO SEGUNDO. Disposiciones Complementarias
Capítulo I Lineamientos secundarios
Artículo Octavo Instancias Participantes.
Artículo Noveno Mecánica Operativa.
Artículo Décimo Evaluación.
Artículo Décimo Primero Indicadores.
Artículo Décimo Segundo Seguimiento, Control y Auditoría.
Artículo Décimo Tercero Transparencia y Contraloría Social
Artículo Décimo Cuarto Perspectiva de Género
Artículo Décimo Quinto Casos de Emergencia o Desastre.
Artículo Décimo Sexto Derechos de las Personas Beneficiarias.
Artículo Décimo Séptimo Obligaciones de las Personas Beneficiarias.
Artículo Décimo Octavo Causas de Baja.
Artículo Décimo Noveno Peticiones o Denuncias.
Artículo Vigésimo Solicitudes de Información
Artículo Vigésimo Primero Compras Sociales.
Transitorios
A N E X O S
Anexo I. Ficha Socioeconómica del Actor Social y Comunitario Venta de Leche en Polvo del Programa de Abasto Social.
Anexo II. Lineamientos, Derechos y Obligaciones para el uso de la tarjeta de dotación de leche Liconsa.
Anexo III. Promotoría Social.
Anexo IV. Convenio para el suministro de leche en polvo.
Anexo V. Convenio modificatorio al convenio para el suministro de leche en polvo.
Anexo VI. Avance Físico y Financiero 2020.
Anexo VII. Presupuesto Ejercido Entregado o Dirigido a las Personas Beneficiarias.
Anexo VIII. Indicadores de Reglas de Operación 2020 del Programa de Abasto Social de Leche.
Anexo IX. Esquema de Contraloría Social.
Anexo X. Información Socioeconómica.
Anexo XI. Cuestionario Único de Actores Sociales y Comunitarios.
Anexo XII. Flujograma para Solicitar la incorporación al Padrón de Beneficiarios.
Anexo XIII. Flujograma para Solicitar Nuevos Puntos de Venta.
Anexo XIV. Flujograma Convenios con Actores Sociales y Comunitarios.
Anexo XV. Flujograma Convenio Modificatorio con Actores Sociales y Comunitarios.
TITULO PRIMERO. Disposiciones Generales
Capítulo I Lineamientos cardinales
Artículo 1º. Establecimiento de las Reglas de Operación de Liconsa, S.A. de C.V.
El presente Acuerdo tiene como objeto establecer las Reglas de Operación que estarán vigentes en el Ejercicio Fiscal 2020, para la ejecución del Programa de Abasto Social de Leche.
Las cifras más recientes de pobreza publicadas por el Consejo Nacional de Evaluación de la Política de Desarrollo Social (CONEVAL) muestran que, en 2016, 53.4 millones de personas se encontraban en condición de pobreza, 62.0 millones de personas presentaban un ingreso inferior a la Línea de Bienestar y 24.6 millones de personas presentaban la carencia de acceso a la alimentación.
Artículo 2º. Objetivo General del Programa.
Contribuir al bienestar social mediante el mejoramiento en el acceso a la alimentación de las personas integrantes de los hogares beneficiarios.
El Programa de Abasto Social de Leche (en lo sucesivo PASL) genera complementariedades y sinergias con otros programas de la SADER que realizan acciones para garantizar el derecho de acceso a la alimentación.
Artículo 3º. Objetivo específico.
Mejorar el acceso a la alimentación de las personas integrantes de los hogares beneficiarios, mediante el acceso al consumo de leche fortificada, de calidad y bajo precio.
Artículo 4º. Población Objetivo.
La población objetivo del programa pertenece a cualquiera de los siguientes grupos:
I. Niñas y niños de 6 meses a 12 años de edad.
II. Mujeres y hombres adolescentes de 13 a 15 años.
III. Mujeres en período de gestación o lactancia.
IV. Mujeres de 45 a 59 años.
V. Personas con enfermedades crónicas y personas con discapacidad.
VI. Personas adultas de 60 y más años.
Dicha población se atiende a través de dos modalidades: Abasto Comunitario y Convenios con Actores Sociales y Comunitarios, considerando que pueden existir asociaciones de personas indígenas y de vecinos que se organizan para tener acceso a los apoyos.
El Programa tendrá como prioridad, para ser beneficiarios, a las personas que habiten en zonas de población mayoritariamente indígena, zonas con mayor grado de marginación o zonas con altos índices de violencia, según los mecanismos establecidos por la Secretaría de Bienestar.
También podrán incorporarse al Programa aquellas personas identificadas mediante visitas domiciliarias y entrevistas casa por casa, recorridos y trabajo de campo realizados por los Servidores de la Nación para el Censo de Bienestar, que cumplan con los requisitos necesarios y sean parte de la población objetivo para poder recibir el beneficio del programa.
Artículo 5º. Cobertura.
El Programa opera a nivel nacional en las 32 entidades federativas en dos modalidades:
I. Abasto Comunitario: concesiones, centros de distribución mercantil y sistema de tiendas Diconsa.
Los puntos de venta se pueden consultar en la página electrónica http://www.gob.mx/liconsa/documentos/puntos-de-venta-liconsa
II. Convenios con Actores Sociales y Comunitarios: Instituciones públicas o personas morales legalmente constituidas sin fines de lucro.
Artículo 6º. Requisitos Generales para el Otorgamiento de los apoyos para la dotación de leche.
I. Abasto Comunitario
Para tener acceso al apoyo del Programa se deberá cumplir con lo siguiente:
| Criterios | Requisitos |
| a. En todos los casos se deberá cumplir con lo siguiente: | |
| i. Que el domicilio del hogar se encuentre dentro de la cobertura del Programa y que en el mismo existan personas con las características de la población objetivo señalada en el artículo 4. | ii. La persona interesada presentará en el punto de venta los siguientes documentos en original o copia para revisión. A. Cualquier identificación Oficial o documento que lo acredite y la "Tarjeta del Bienestar" B. Comprobante de domicilio, que puede ser: recibo de luz, agua, predial o teléfono; en su caso, escrito libre de la autoridad local en el que se valide la residencia de la persona solicitante. El comprobante deberá ser de fecha reciente (antigüedad máxima de tres meses). C. Acta de nacimiento de la persona titular y de las personas beneficiarias. D. Clave Única del Registro de Población (CURP) de la persona titular y de las personas beneficiarias. |
| b. Adicionalmente a lo señalado en el inciso a), las mujeres en período de gestación o lactancia deberán: | |
| i. Acreditar que se encuentra en periodo de gestación o lactancia. | i. Presentar constancia médica o, en su caso, copia del carnet perinatal y/o control de embarazo u otro documento expedido por instituciones de salud del Gobierno Federal, estatal, municipal u otra institución de salud, en la que haga referencia a su situación de embarazo, o ii. Presentar acta de nacimiento o constancia de alumbramiento del recién nacido. |
| c. Adicionalmente a lo señalado en el inciso a), las personas con enfermedades crónicas y personas con discapacidad deberán: | |
| i. Comprobar ser persona con enfermedad crónica o persona con discapacidad que requiera incluir leche en su dieta. | i. Presentar constancia médica oficial expedida por instituciones de salud del gobierno federal, estatal, municipal u otra institución de salud en la que se recomiende ingerir leche. |
II. Convenios con Actores Sociales y Comunitarios
Para celebrar convenios con Actores Sociales y Comunitarios se deberá cumplir con lo siguiente:
| Criterios | Requisitos |
| a. Acreditar el Objeto del Actor Social y Comunitario solicitante. | La persona representante del Actor Social y Comunitario presentará en el centro de trabajo por escrito la solicitud de suscripción de convenio para el suministro de leche en polvo, anexando copia del acta constitutiva, cuyo objeto social sin fines de lucro deberá relacionarse al apoyo alimentario. |
| b. Acreditar el número de personas beneficiarias. | El Actor Social y comunitario, presentará el padrón de personas que atiende, por entidad federativa y centros de atención. |
| c. Acreditar su inscripción en el Registro Federal de Organizaciones de la Sociedad Civil. | Las organizaciones de la sociedad civil, presentarán copia de la Clave Única de Inscripción denominada CLUNI. |
| d. Acreditar la operatividad del Actor Social y Comunitario. | El centro de trabajo formulará al Actor Social y Comunitario, la ficha socioeconómica del Anexo 1, con excepción de las Instituciones Gubernamentales. |
III. Criterios de Selección
a. Abasto comunitario
Las personas que se incorporen al padrón de Beneficiarios de LICONSA serán las que se encuentren en las Zonas de Atención Prioritaria y las demás que comunique la Secretaría de Bienestar con base a los acuerdos que se establezcan con SEGALMEX y Liconsa para el censo del Bienestar; lo anterior estará sujeto a la suficiencia presupuestal del Programa y de la disponibilidad de leche.
El Programa prevé que en caso de situaciones inesperadas o fortuitas en donde el suministro de leche sea insuficiente tendrán prioridad de atención los niños y las niñas de 6 meses hasta 5 años y mujeres en periodo de gestación y lactancia, con la finalidad de prevenir problemas nutricionales y apoyar su desarrollo.
Los beneficios del Programa se entregarán de manera directa y sin intermediarios a los beneficiarios, por la Unidad Responsable de la ejecución, preferiblemente por instrumento bancario.
En el caso de tratarse de asociaciones, se priorizará a las asociaciones comunitarias indígenas y de vecinos.
b. Convenios con Actores Sociales y Comunitarios
Los Actores Sociales y Comunitarios son una agrupación de personas con un fin determinado, legalmente constituidas bajo la figura jurídica de persona moral con objeto social y/o comunitario sin fines de lucro.
Son convenios con Actores Sociales y Comunitarios los que atienden a personas en situación de vulnerabilidad y que son validados a través de la ficha socioeconómica que aplique el centro de trabajo, actas de asamblea, actas y constancias vecinales o representaciones de pueblos indígenas, de acuerdo a las siguientes prioridades:
i. Personas que pertenecen a los mismos grupos considerados en la población objetivo.
ii. Personas que por diferentes situaciones están ingresadas en alguna institución pública o privada de asistencia social.
iii. Personas que son apoyadas por instituciones privadas de asistencia social que suman esfuerzos con el gobierno federal, estatal y/o municipal a favor de la nutrición de las niñas y los niños, así como de la población objetivo.
El Programa prevé que en caso de situaciones inesperadas o fortuitas en donde el suministro de leche sea insuficiente, tendrán prioridad:
i. Asociaciones que atiendan a grupos que habitan en zonas con alto porcentaje de personas en situación de pobreza.
ii. Asociaciones que se encuentren ubicadas en zonas rurales o indígenas con alto porcentaje de población en situación de pobreza y aquellas que se encuentran en zonas con alto índice de inseguridad.
iii. Asociaciones que atiendan a niños y a niñas de hasta 12 años y adultos mayores que habiten en zonas con alto porcentaje de personas en situación de pobreza.
Artículo 7º. Tipos y Montos de Apoyo.
El Programa otorga una dotación de leche fortificada y con alto valor nutricional, a un precio preferencial por litro, transfiriendo un margen de ahorro al hogar beneficiario, generado por la diferencia entre el precio de la leche Liconsa y el de la leche comercial.
I. Abasto Comunitario
La dotación de leche autorizada es de hasta cuatro litros a la semana por persona beneficiaria
registrada en el padrón y cada hogar tendrá derecho a adquirir un máximo de 24 litros a la semana, el Consejo de Administración de Liconsa definirá el rango de precios aplicables en el territorio Nacional, dependiendo del número de personas beneficiarias, conforme a lo que se establece en el siguiente cuadro, previa presentación de la tarjeta de dotación de leche:
| Número de personas Beneficiarias | Dotación semanal (litros) |
| 1 | 4 |
| 2 | 8 |
| 3 | 12 |
| 4 | 16 |
| 5 | 20 |
| 6 o más | 24 |
II. Convenios con Actores Sociales y Comunitarios (beneficiarios)
El esquema de operación para la dotación de leche en polvo, se especifica en el convenio suscrito con el Actor Social y comunitario, de acuerdo a las necesidades y características operativas de las partes involucradas.
Se podrán celebrar convenios modificatorios a los convenios suscritos con Actores Sociales y Comunitarios para ajustar, entre otros términos, el número de personas beneficiarias, el suministro por día autorizado y el representante legal.
La cobertura de los convenios no podrá rebasar el cuatro por ciento del total del padrón de beneficiarios.
Para la determinación de los beneficiarios del Programa se atenderán las reglas establecidas en los artículos anteriores, que van del número 4 a este 7, así como los datos que arroje el Censo del Bienestar.
El Padrón del Bienestar está integrado con los beneficiarios de los Programas Integrales para el Desarrollo con información de las dependencias y entidades responsables, información de entrevistas domiciliarias, de visitas de campo y del registro e inscripción por los medios específicos para cada programa.
El Padrón del Bienestar permitirá implementación de acciones transversales de las distintas dependencias de la Administración Pública Federal que faciliten la planeación, coordinación y ejecución de los programas.
El Padrón del Bienestar será revisado por la Secretaría de la Función Pública de manera continua para su debida validación, actualización y auditoría, atendiendo los criterios de Zonas de Atención Prioritaria y los demás que la Secretaría de Bienestar defina.
TITULO SEGUNDO. Disposiciones Complementarias
Capítulo I Lineamientos secundarios
Artículo 8º. Instancias Participantes
I. Instancias Ejecutoras
Para el correcto cumplimiento de sus objetivos LICONSA regirá sus actividades por los lineamientos, políticas directrices y demás reglas que le indique Seguridad Alimentaria Mexicana-SEGALMEX-.
Los centros de trabajo de LICONSA dentro de su ámbito territorial, son los responsables de la operación del Programa y del cumplimiento de las presentes Reglas de Operación y la normatividad aplicable en la materia.
II. Instancia Normativa
LICONSA será instancia normativa del Programa y estará facultada para interpretar las presentes Reglas y resolver sobre aspectos no contemplados en ellas.
LICONSA contará con el apoyo técnico en materia de derechos humanos e igualdad de género con objeto de atender cualquier situación relacionada con estos temas, promoviendo siempre el principio de igualdad sustantiva.
El Director General de LICONSA tendrá amplias facultades para la interpretación y aclaración de dudas o necesidades respecto de estas Reglas de Operación y para decidir todo lo necesario para su adecuado cumplimiento. También podrá conocer y resolver todas aquellas cuestiones no previstas en ellas.
III. Coordinación Interinstitucional
La coordinación institucional y vinculación de acciones buscará potenciar el impacto de los recursos, fortalecer la cobertura de las acciones, detonar la complementariedad y reducir gastos administrativos. Con este mismo propósito, podrá establecer acciones de coordinación con los gobiernos de las entidades federativas, y de los municipios, las cuales tendrán que darse en el marco de las disposiciones de las presentes Reglas de Operación y de la normatividad aplicable; y verificar que dichas acciones no se contrapongan, afecten o presenten duplicidades con otros programas o acciones del gobierno federal.
LICONSA podrá tomar las decisiones necesarias que permitan la concurrencia de acciones y presupuesto en los programas de desarrollo regional que, en el marco de las disposiciones de las presentes Reglas de Operación y de la normatividad aplicable.
Artículo 9º. Mecánica Operativa
I. Proceso de Operación
a. Incorporación al padrón de beneficiarios
i. Abasto Comunitario
A. La persona interesada en adquirir la leche deberá presentar los documentos indicados en el artículo 6º. de estas Reglas de Operación al personal de promotoría social en el punto de venta, de conformidad con el día y horario de visitas colocados en los mismos. Anexo X.
B. El personal de promotoría social cotejará la documentación y le informará a la persona solicitante en ese momento si falta algún documento, de ser así deberá presentar la documentación completa para realizar su trámite en la siguiente visita del personal de promotoría social al punto de venta.
C. El personal de promotoría social informará a la persona representante del hogar en el punto de venta el resultado de su gestión para su incorporación al padrón de beneficiarios. En el caso de una respuesta afirmativa, se le entregará a la persona solicitante su tarjeta de dotación de leche, en un plazo de hasta 30 días naturales posteriores a la fecha de aceptación.
D. El personal de promotoría social realizará las funciones referidas en el Anexo III.
ii. Convenios con Actores Sociales y Comunitarios
E. Los Actores Sociales y Comunitarios interesados deberán presentar por escrito en el centro de trabajo, la solicitud de convenio para el suministro de leche en polvo y entregar los documentos indicados en el artículo 6º.
F. Si los Actores Sociales y Comunitarios cumplen con la normatividad aplicable, se autorizará la suscripción del convenio de suministro de leche en un plazo de hasta 90 días naturales posteriores a la fecha de presentación de la solicitud, con base en el esquema de operación que se acuerde y el modelo de Convenio establecido en el Anexo IV.
G. El Actor Social y Comunitario en el momento de hacer su requerimiento, enviará al centro de trabajo el número de personas beneficiarias.
H. El Actor Social y Comunitario enviará al centro de trabajo, el padrón de personas beneficiarias atendidas en los primeros cinco días naturales del mes siguiente de la entrega de leche por parte de LICONSA.
I. En el caso de ajuste del número de personas beneficiarias, del suministro de leche en polvo por día autorizado y/o cambio de la persona representante legal, entre otros
términos, se celebrará convenio modificatorio, conforme al modelo establecido en el Anexo V.
b. Instalación de puntos de venta para abasto comunitario.
i. Las instancias de gobierno o alguna persona en representación de la comunidad interesada en la instalación de un punto de venta, podrán presentar la solicitud en cualquier día y hora hábiles, en el centro de trabajo de LICONSA o en cualquier punto de venta, con el personal de promotoría social, de acuerdo a lo estipulado en el siguiente inciso de estas Reglas. Si existiera algún faltante en las información o documentación, en ese momento se le informará a la persona solicitante, quién, al contar con la información completa, podrá reiniciar el procedimiento.
La ubicación de los centros de trabajo, puede consultarse en el sitio
http://www.gob.mx/tramites/ficha/instalacion-de-nuevos-puntos-de-venta-de-leche-del-programa-de-abasto-social-de-leche-a-cargo-de-liconsa/LICONSA1472
ii. El centro de trabajo efectuará un análisis de las características de la zona mediante el levantamiento del estudio de factibilidad, con el propósito de verificar el cumplimiento de los siguientes requisitos para la instalación de puntos de venta y dictaminar su procedencia:
| Criterios | Requisitos |
| Que exista interés de la población para la instalación de un punto de venta. | Las instancias de gobierno o alguna persona en representación de la comunidad deberán presentar en el centro de trabajo correspondiente, una solicitud de instalación de punto de venta LICONSA mediante escrito libre, en la cual se indique el nombre y domicilio de la organización y/o persona solicitante, además de los datos de la ubicación donde se busca instalar el punto de venta. Deberá existir una distancia mínima de 2 km. de desplazamiento físico, entre el punto central de la zona donde habiten las posibles personas beneficiarias y los puntos de venta en operación. Los domicilios de los centros de trabajo podrán consultarse en http://www.gob.mx/tramites/ficha/instalacion-de-nuevos-puntos-de-venta-de-leche-del-programa-de-abasto-social-de-leche-a-cargo-de-liconsa/LICONSA1472 |
| Contar con un mínimo de posibles personas que se beneficien | El número mínimo de posibles personas beneficiarias debe ser de 300 para leche líquida; para leche en polvo será de 200 en localidades mayores de 2,500 habitantes y de 100 para localidades menores. En el caso de Zonas de Atención Prioritaria, estas cantidades mínimas no serán limitantes para llevar a cabo una instalación |
| Asegurar la existencia de un local, comercio particular o tienda comunitaria de DICONSA. | El inmueble debe contar con las características, capacidad e higiene adecuadas, de acuerdo con la cantidad y tipo de leche a expender y que haya accesibilidad de caminos para los vehículos que transportan la leche. |
iii. La persona solicitante apoyará, de manera corresponsable, al centro de trabajo en el levantamiento de la información para realizar el estudio de factibilidad y la obtención del local adecuado para la operación.
iv. En caso de que se dictamine la procedencia de instalar un nuevo punto de venta, el centro de trabajo enviará el estudio de factibilidad a la oficina central para su validación. Se dará respuesta escrita al solicitante en un plazo no mayor de 90 días naturales después de haber recibido su solicitud.
v. La instalación del punto de venta estará sujeta a la disponibilidad presupuestal, a las metas de padrón y de leche, así como a las rutas de promotoría social y de distribución de
leche, de acuerdo a la normatividad interna.
vi. La distancia mínima de 2 km. de desplazamiento físico, podrá ser menor, por las siguientes condiciones:
A. La existencia de avenidas o carreteras que pongan en riesgo la integridad física de las personas beneficiarias, al intentar cruzar o transitarlas.
B. El relieve o condiciones climáticas, que dificulten el deslazamiento de las personas beneficiarias.
C. Insuficiencia de alumbrado o presencia de zonas delictivas en el trayecto recorrido por las personas beneficiarias, desde sus domicilios hasta el punto de venta.
D. Alta densidad de población objetivo, que afecte la eficacia en la atención en los puntos de venta.
E. Cuando se requiera atender a un grupo de personas beneficiarias con leche líquida y a otro con polvo.
c. Entrega del beneficio
i. La leche se entrega a los hogares beneficiarios de la modalidad de abasto comunitario, por medio de los siguientes puntos de venta:
A. Puntos de venta: establecimientos operados por personas físicas que en su mayoría distribuye la leche líquida, y sus inmuebles son generalmente proporcionados por los gobiernos locales.
B. Tiendas particulares: establecimientos operados por personas físicas con pequeños comercios que trabajan con limitado surtido de mercancías y que en su mayoría distribuyen la leche en polvo.
C. Tiendas comunitarias de DICONSA: establecimientos que distribuyen solamente leche en polvo.
Cuando las personas beneficiarias eventualmente no asistan a los puntos de venta de leche líquida el día que les corresponde retirar su dotación y en consideración a que este tipo de leche es altamente perecedera y no puede almacenarse ni devolverse, una vez que concluya el horario de venta, se podrá vender a quien la requiera.
En caso de que el hogar beneficiario cambie de domicilio, la persona representante del hogar deberá informar verbalmente al personal de promotoría social, de conformidad con el día y horario de visitas colocados en el punto de venta más cercano, presentando un comprobante del nuevo domicilio. Asimismo, en caso de extravío de la tarjeta de dotación, se deberá informarlo al personal de promotoría social para que le haga entrega de la nueva tarjeta en un plazo de hasta 60 días naturales posteriores a la fecha de la notificación de dicha pérdida.
Cuando se cierre un punto de venta, se tratará de no afectar a su población beneficiaria, la cual será adscrita a otros puntos de venta cercanos.
ii. En la modalidad de convenios con Actores Sociales y Comunitarios la leche en polvo se distribuye por medio de los siguientes canales:
A. La infraestructura de distribución de LICONSA.
B. En los centros de trabajo de LICONSA.
De acuerdo con su forma de operación, cada Actor Social y Comunitario hará llegar la leche a las personas beneficiarias que atiende.
De acuerdo con lo dispuesto en el Artículo 75, fracción VI, de la Ley Federal de Presupuesto y Responsabilidad Hacendaria, LICONSA continuará desarrollando estrategias para fortalecer sus fuentes alternativas de ingresos, con el fin de lograr una mayor autosuficiencia financiera. SEGALMEX, de conformidad con el Artículo Tercero de su Estatuto Orgánico, cuidará, en todo momento, que no falten a LICONSA los elementos necesarios y el abasto para el cumplimiento de su función social.
II. Registro de Operaciones
a. Ejercicio y aprovechamiento de los recursos
Para lograr un mejor nivel de ejercicio y aprovechamiento de los recursos, LICONSA realizará una calendarización eficiente; asimismo, preverá que las aportaciones que en su caso se realicen, se ejerzan de manera oportuna y en apego a la normatividad aplicable.
Adicionalmente, a partir del 30 de junio la SADER podrá realizar una evaluación del avance de las acciones y ejercicio de los recursos en cada entidad. Los recursos que no hubieren sido ejercidos o comprometidos, o cuyas acciones no tuvieran avance de acuerdo a lo programado, serán reasignados por LICONSA.
Asimismo, LICONSA, entregará reportes acumulados trimestrales en archivos electrónicos a través de los medios disponibles a la SHCP, SFP y Cámara de Diputados, en el último día hábil de los meses de abril, julio y octubre del ejercicio fiscal vigente y en enero del año subsecuente. Anexo VII.
b. Avances físico-financieros
LICONSA presentará trimestralmente a la Secretaría de Hacienda y Crédito Público (SHCP), el informe sobre el avance físico y financiero de las metas programadas. Anexo VI.
c. Cierre de ejercicio
LICONSA integrará el cierre de ejercicio anual del programa y lo remitirá debidamente validado en medios magnéticos y/o electrónicos, a la Secretaría de la Función Pública (SFP), a más tardar el último día hábil del mes de enero del ejercicio fiscal subsecuente.
Artículo 10º. Evaluación.
Con la finalidad de identificar y atender posibles áreas de mejora en el diseño, gestión y resultados del Programa, LICONSA realizará las evaluaciones externas, de acuerdo con los plazos y términos previstos en la Ley Federal de Presupuesto y Responsabilidad Hacendaria, en los "Lineamientos generales para la evaluación de los Programas Federales de la Administración Pública Federal" y en la normatividad aplicable vigente, publicando los resultados a través del portal de Internet de LICONSA: http://www.gob.mx/liconsa.
Con fundamento en el artículo 59, fracción XI, de la Ley Federal de las Entidades Paraestatales, LICONSA deberá presentar al Consejo de Administración, por lo menos dos veces al año, informes de autoevaluación.
Artículo 11º. Indicadores
Los indicadores de Propósito y Componente de la Matriz de Indicadores para Resultados (MIR) del Programa están contenidos en el anexo VIII de las presentes Reglas de Operación. La información correspondiente a estos indicadores será reportada por LICONSA en el Portal Aplicativo de la Secretaría de Hacienda y Crédito Público (PASH).
Artículo 12º. Seguimiento, Control y Auditoría.
Con el propósito de corroborar la correcta operación del programa, LICONSA llevará a cabo el seguimiento al ejercicio de los recursos asignados al mismo, así como a las acciones ejecutadas, resultados, indicadores y metas alcanzadas.
I. Seguimiento físico y operativo
El Programa deberá realizar un ejercicio de seguimiento físico y operativo de sus apoyos, acciones o servicios entregados, cuya metodología deberá ser elaborada con base en los elementos técnicos mínimos que defina LICONSA. Asimismo, se establecerá el mecanismo para la validación de dicha metodología, previo a su aplicación en campo y revisará el informe final del ejercicio, analizando su consistencia metodológica y sus resultados.
II. Control y Auditoría
Los ejecutores serán responsables de la supervisión directa de las obras, proyectos o acciones, así como de verificar que en su ejecución se cumpla la normatividad aplicable, mientras que las Unidades Responsables del Programa de la Secretaría de Agricultura y Desarrollo Rural (SADER) en
las entidades federativas serán responsables de supervisar y verificar el avance y la correcta terminación y entrega de las obras, proyectos y/o acciones, así como de solicitar la comprobación documental del gasto ejercido debidamente certificada, en los plazos establecidos en las Reglas de Operación, dejando evidencia de la confirmación de su autenticidad en los medios electrónicos implementados por la autoridad fiscal y asegurar su debido resguardo. Considerando que los recursos federales de este Programa, ejecutados por las entidades federativas o sus municipios no pierden su carácter federal al ser entregados a los mismos, su ejercicio está sujeto a las disposiciones federales aplicables y podrán ser auditados en el marco del Sistema Nacional de Fiscalización por las siguientes instancias, conforme a la legislación vigente y en el ámbito de sus respectivas competencias: por la Auditoría Superior de la Federación; por el Órgano Interno de Control en la Secretaría de Agricultura y Desarrollo Rural (SADER); por la Secretaría de la Función Pública (SFP) en coordinación con los órganos de control de los gobiernos locales.
La instancia Ejecutora dará todas las facilidades a dichas Instancias Fiscalizadoras para realizar las auditorías, revisiones o visitas de inspección, de acuerdo a los programas anuales de auditorías o en el caso que lo juzgue pertinente. Asimismo, efectuarán las acciones necesarias para dar atención a las recomendaciones planteadas por dichas instancias fiscalizadoras, independientemente de las sanciones a que hubiere lugar, por la inobservancia de esta disposición la Unidad Responsable del Programa determinará con base en lo anterior si suspende o limita la ministración de los recursos federales en el siguiente ejercicio presupuestal.
Artículo 13º. Transparencia y Contraloría Social
Se promoverá la participación de las personas beneficiarias del Programa de Abasto Social de Leche a través de la integración y operación de Comités de Beneficiarios, para el seguimiento, supervisión y vigilancia del cumplimiento de las metas y acciones comprometidas en el mismo, así como de la correcta aplicación de los recursos públicos asignados.
Estas Reglas de Operación, además de su publicación en el Diario Oficial de la Federación, están disponibles para su consulta en la página electrónica de LICONSA: www.liconsa.gob.mx
Artículo 14º. Perspectiva de Género
En el ámbito de su competencia, el Programa deberá incorporar acciones de carácter temporal (acciones afirmativas) que permitan a las mujeres el pleno ejercicio de los derechos sociales de manera igualitaria.
Como parte de este esfuerzo, el Programa incluye entre su población objetivo a niñas de 6 meses a 12 años de edad; mujeres de 13 a 15 años y mujeres de 45 a 59 años para prevenir problemas de salud específicos al sexo femenino. Asimismo, se atiende a mujeres en periodo de gestación y lactancia para contribuir a la buena salud y nutrición tanto de la madre como de sus hijas(os) así como a mujeres a partir de 60 años.
Artículo 15º. Casos de Emergencia o Desastre.
Para facilitar la continuidad de los apoyos otorgados a las personas beneficiarias, el Programa elaboró y definió el protocolo para casos de emergencia o desastre, al que deberá dar cumplimiento el programa en los casos que lo amerite. El Protocolo podrá ser consultado en la siguiente liga: https://www.gob.mx/cms/uploads/attachment/file/412460/Protocolo_en_caso_de_emergencia_final_23_05_2018_pdf.pdf.
Artículo 16º. Derechos de las Personas Beneficiarias.
I. Recibir un trato digno, respetuoso, oportuno, con calidad y equitativo, sin discriminación alguna.
II. Solicitar y recibir gratuitamente información acerca del Programa.
III. Recibir una tarjeta personalizada con la información del representante del hogar.
IV. Adquirir la cantidad de leche que les sea autorizada, con base en el artículo 7, Fracción I.
V. Tolerancia máxima de cinco minutos en el horario establecido para la venta de leche líquida.
VI. Recibir la dotación de leche sin condicionamiento a la compra de otros productos.
VII. Obtener una nueva tarjeta por cambio de domicilio, extravío de la tarjeta o por registro de una nueva persona beneficiaria, previo aviso al personal de promotoría social, entrega de los datos
correspondientes y devolución de la tarjeta, excepto en el caso de extravío.
VIII. Presentar quejas o denuncias por irregularidades en el servicio.
Artículo 17º. Obligaciones de las Personas Beneficiarias.
I. No transferir la tarjeta, no tener más de una, no venderla o hacer mal uso de la misma.
II. Presentar la tarjeta para comprar la leche y cuando le sea solicitada por personal autorizado.
III. Conservar la tarjeta en buen estado y entregarla a solicitud del personal de promotoría social a cambio de la nueva.
IV. Destinar la leche exclusivamente al consumo de los integrantes del hogar.
V. No provocar desórdenes, no realizar propaganda ni proselitismo político o religioso en el punto de venta.
VI. No celebrar actos que alteren o impidan el suministro y venta de la leche.
VII. Notificar verbalmente al personal de promotoría social respecto a los cambios de domicilio y extravío de la tarjeta en los días señalados en los carteles que se colocan en los puntos de venta.
VIII. Asistir en los días y horarios que les corresponda retirar su dotación.
IX. Acudir con el personal de promotoría social para los pases de lista, canjes de tarjeta, operativos de actualización y depuración del padrón, en los horarios que se den a conocer en los puntos de venta para alguna o varias de las acciones que se mencionan.
X. Cumplir con los demás lineamientos, derechos y obligaciones para el uso de la tarjeta de dotación de leche LICONSA, establecidos en el reverso de la misma, contenidos en el Anexo II.
Artículo 18º. Causas de baja.
La baja parcial tiene lugar cuando una o más personas beneficiarias de un hogar registrado salen del padrón, pero conserva al menos una persona beneficiaria activa en el mismo. La baja total se da cuando salen todos los beneficiarios de un hogar del padrón.
Las causales de baja del padrón y la consecuente cancelación de la dotación de leche son:
I. A partir de que cumplan 16 años, las personas beneficiarias del grupo de mujeres y hombres adolescentes de 13 a 15 años.
II. Un año después de que las mujeres en gestación o lactancia se incorporaron al padrón.
III. Por fallecimiento o retiro voluntario de las personas beneficiarias.
IV. Cuando las personas integrantes del hogar no acudan a recoger su dotación de leche líquida durante un período mayor de 30 días naturales y un período de 90 días naturales en el caso de dotación de leche en polvo.
V. Por incumplir con los lineamientos y obligaciones impresos en el reverso de la tarjeta.
VI. Cuando las personas titulares de las tarjetas de dotación de leche hayan proporcionado información socioeconómica falsa.
VII. Cuando las personas integrantes del hogar presten o vendan la tarjeta de dotación.
VIII. Por destinar a fines distintos al consumo la leche que es sólo para las personas integrantes del hogar.
IX. Cuando LICONSA detecte duplicidad de registros, derivado del cotejo de información del padrón en los centros de trabajo.
Artículo 19º. Peticiones o denuncias.
Se podrán presentar en:
I. Órgano Interno de Control en LICONSA:
Para recepción de denuncias Teléfono:
Larga distancia sin costo: 800-882-2676
Correo electrónico: rrojasu@liconsa.gob.mx; quejas.liconsa@yahoo.com.mx
Página Web: Realiza tu denuncia en línea aquí:
https://www.gob.mx/tramites/ficha/presentacion-de-quejasy-denuncias-en-la-sfp/SFP54
Domicilio: Ricardo Torres #1 Fracc. Lomas de Sotelo, C.P. 53390, Naucalpan, Estado de México.
II. En la Secretaría de la Función Pública
Ciudad de México y Área Metropolitana:
Teléfono: 2000-3000
Larga distancia sin costo: 800-3862-466
De Estados Unidos 800-4752-393
Correo electrónico: contactociudadano@funcionpublica.gob.mx
Página electrónica: www.funcionpublica.gob.mx
Domicilio: Insurgentes Sur 1735, Colonia Guadalupe Inn, Alcaldía Álvaro Obregón, Código Postal 01020, Ciudad de México.
III. Coordinaciones Generales de LICONSA, a través del BUZÓN colocado para tal efecto.
También, se pone a disposición de la ciudadanía la posibilidad de la presentación de denuncias para reportar hechos, conductas, situaciones o comportamientos, se puede consultar en la página www.conamer.gob.mx, con la Homoclave: SADER.
Artículo 20º. Solicitudes de Información.
Las solicitudes de información podrán realizarse ante el Área de Atención Ciudadana, por escrito y/o vía telefónica, a través de:
I. LICONSA: Área de Atención Ciudadana
Teléfonos: 55-5237-9100
Larga distancia sin costo: 800-800-6939
Correo electrónico: rrojasu@liconsa.gob.mx; quejas.liconsa@yahoo.com.mx
Domicilio: Ricardo Torres #1, Fracc. Lomas de Sotelo, C.P. 53390, Naucalpan, Estado de México
Las quejas y denuncias podrán realizarse por escrito y/o vía telefónica, a través de: rrojasu@liconsa.gob.mx
| | Teléfono | Correo y página electrónica | Domicilio |
| Secretaría de la Función Pública | Larga distancia sin costo: 800 386 2466 de la Ciudad de México, y área metropolitana. De Estados Unidos: 800 475 2393 | contactociudadano@funcionpublica.gob.mx | Insurgentes Sur 1735, Col. Guadalupe Inn, Alcaldía Álvaro Obregón, C.P. 01020, Ciudad de México |
Artículo 21º. Compras sociales.
Para cumplir con el Programa de Abasto Social de Leche, se abastecerá en primer término de pequeños productores que posean de 1 a 35 vacas y medianos productores de 36 a 100 vacas limitado a 25 litros por vaca diarios. Cuando exista precio de garantía el mismo se aplicará exclusivamente a los productores de leche antes mencionados. Para dar continuidad y certeza de que estas condiciones se cumplan, LICONSA revisará periódicamente su padrón de productores.
Cuando las adquisiciones a los anteriores productores no sean suficientes, LICONSA podrá comprar leche fluida a productores que rebasen los límites de vacas antes señalados, y los límites de litros por vaca, enunciados en el párrafo anterior, pero, en tal caso, lo hará a precio comercial. Igualmente podrá surtirse a través de importaciones cumpliendo con la normatividad respectiva. En lo referente a la calidad, en todos los casos se estará a lo dispuesto en las normas oficiales establecidas.
Para las actividades de recepción se usará una herramienta tecnológica que incremente los controles. Tanto los transportistas como el personal del Centro de Acopio deberán descargar la aplicación móvil que les proporcione la Dirección de Operaciones de LICONSA.
Para el detalle de las operaciones de entrega y recepción de leche fluida la propia Dirección emitirá los lineamientos a seguir.
TRANSITORIOS
PRIMERO.- El presente Acuerdo entrará en vigor el día de su publicación en el Diario Oficial de la Federación.
SEGUNDO.- Se abroga el Acuerdo por el que se emiten las Reglas de Operación del Programa de Abasto Social de Leche, a cargo de Liconsa, S.A. de C.V., para el ejercicio fiscal 2019, publicado en el Diario Oficial de la Federación el primero de marzo del mismo año y el Acuerdo modificatorio publicado en el Diario Oficial de la Federación el ocho de abril de dos mil diecinueve.
TERCERO.- LICONSA seguirá utilizando la infraestructura operativa que sirva de apoyo en la selección de los Beneficiarios del Programa de Abasto Social de Leche, así como las herramientas tecnológicas para poder ordenar las actividades, en tanto se alinea a las disposiciones de operación del Censo del Bienestar.
Ciudad de México, a 31 de diciembre de 2019.- El Secretario de Agricultura y Desarrollo Rural, Víctor Manuel Villalobos Arámbula.- Rúbrica.
 | ANEXOS Anexo I |
DIRECCIÓN DE ABASTO SOCIAL
FICHA SOCIOECONÓMICA DEL ACTOR SOCIAL Y COMUNITARIO
VENTA DE LECHE EN POLVO DEL PROGRAMA DE ABASTO SOCIAL
| Centro de Trabajo: | | | | | | | | | | | | | | Fecha de Elaboración: | | | | | | | | | | | ||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | Día | Mes | Año | |||||
| I. IDENTIFICACIÓN |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Razón Social: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Fecha de Constitución: | Año: | | | | | | | | Mes: | | | | | | | Día: | | | | | | | | | | | |||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Clave Única de Inscripción al Registro Federal de las Organizaciones de la Sociedad Civil (CLUNI): | | | | | | | | | | | | | | RFC: | | | | | | | | | | | | | |||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Número de Teléfono: | | | | | | | | | | | Correo Electrónico: | | | | | | | | | | | | | | | ||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| II. DOMICILIO FISCAL |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Tipo de Vialidad: | | | | | Nombre de la Vialidad: | | | | | | | | | | | | | | | | | | | | | ||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | Número Exterior: | | | | | | Letra: | | | | | Número Interior: | | | | | Letra: | | | | | ||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Tipo de Asentamiento Humano: | | | | Nombre del Asentamiento Humano: | | | | | | | | | | | | | | | |||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Código Postal: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Entre Vialidades: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Tipo de Vialidad 1: | | | | | Nombre de la Vialidad: | | | | | | | | | | | | | | | | | | | | |||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Tipo de Vialidad 2: | | | | | Nombre de la Vialidad: | | | | | | | | | | | | | | | | | | | | |||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Vialidad Posterior: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Tipo de Vialidad: | | | | | | Nombre de la Vialidad: | | | | | | | | | | | | | | | | | | | | ||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Descripción de la Ubicación: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Entidad Federativa: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | Clave | | | | | ||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Municipio o Delegación: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | Clave | | | | | ||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Localidad: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | Clave | | | | |||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Ámbito: | | Rural: | | | | | | | | | | | | | Urbano : | | | | | | | | | | | | | | | ||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| II. DOMICILIO GEOGRAFICO |
| | ||||||||||||||||||||||||||||||||||||||
| | ¿El domicilio geográfico corresponde al domicilio fiscal? | | Si | | No | | | | | | | | | | | | | | | |||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||
| | Si la respuesta es "No", continúe con el llenado de esta sección, si la respuesta es "Sí", pase a la Sección IV. | | | | | | | | ||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||
| | Tipo de Vialidad: | | | | | | Nombre de la Vialidad: | | | | | | | | | | | | | | | | | | | | | |||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||
| | | | | Número Exterior: | | | | | | Letra: | | | | | Número Interior: | | | | | Letra: | | | | | ||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||
| | Tipo de Asentamiento Humano: | | | | Nombre del Asentamiento Humano: | | | | | | | | | | | | | | | |||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Código Postal: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Entre Vialidades: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Tipo de Vialidad 1: | | | | | Nombre de la Vialidad: | | | | | | | | | | | | | | | | | | | | |||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Tipo de Vialidad 2: | | | | | Nombre de la Vialidad: | | | | | | | | | | | | | | | | | | | | |||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Vialidad Posterior: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Tipo de Vialidad: | | | | | | Nombre de la Vialidad: | | | | | | | | | | | | | | | | | | | | ||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Descripción de la Ubicación: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Entidad Federativa: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | Clave | | | | | ||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Municipio o Delegación: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | Clave | | | | | ||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Localidad: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | Clave | | | | |||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Ámbito: | | Rural: | | | | | | | | | | | | | Urbano : | | | | | | | | | | | | | | | ||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| IV. DATOS DE LAS PERSONAS INTEGRANTES DEL COMITÉ ADMINISTRATIVO |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | 1.- Nombre: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | Primer Apellido | | Segundo Apellido | | Nombre (s) | | |||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | Cargo: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | CURP: | | | | | | | | | | | | | | | | | | | | RFC: | | | | | | | | | | | | | | ||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | Fecha de Nacimiento: | Año: | | | | | | | | Mes: | | | | | | Día: | | | Sexo: | | | | | | | | ||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | H | | M | | | ||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | Estado de Nacimiento: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | 2.-Nombre: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | Primer Apellido | | Segundo Apellido | | Nombre (s) | | |||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | Cargo: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | CURP: | | | | | | | | | | | | | | | | | | | | RFC: | | | | | | | | | | | | | | |||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Fecha de Nacimiento: | Año: | | | | | | | | Mes: | | | | | | Día: | | | Sexo: | | | | | | | | |||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | H | | M | | | |||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Estado de Nacimiento: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | 3.- Nombre: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | Primer Apellido | | Segundo Apellido | | Nombre (s) | | ||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Cargo: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | CURP: | | | | | | | | | | | | | | | | | | | | RFC: | | | | | | | | | | | | | | |||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Fecha de Nacimiento: | Año: | | | | | | | | Mes: | | | | | | Día: | | | Sexo: | | | | | | | | |||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | H | | M | | | |||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Estado de Nacimiento: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | 4.- Nombre: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | Primer Apellido | | Segundo Apellido | | Nombre (s) | | ||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Cargo: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | CURP: | | | | | | | | | | | | | | | | | | | | RFC: | | | | | | | | | | | | | | |||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Fecha de Nacimiento: | Año: | | | | | | | | Mes: | | | | | | Día: | | | Sexo: | | | | | | | | |||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | H | | M | | | |||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Estado de Nacimiento: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| V. CARACTERÍSTICAS GENERALES DE ATENCIÓN |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | Tipo de organización : | | | Pública | | | | | | | | | | Privada | | | | | | | Mixta | | | | | |||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | Objeto Social del Actor Social: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | Clasificación: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | | | | | Casa-Hogar | | | | | Casa-Cuna | | | | | | | | Internado | | | | | | | | | ||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | | | | | Estancia Infantil | | | | | Asilo de Ancianos | | | | | | Asistencia Médica | | | | | | | ||||||||||||||||||||||||||||||
| | | | | | o Guardería | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | | | | | Trabajo | | | | | | | Albergue | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||
| | | | | | Comunitario | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | | | | | Otro | | | | | | | | Especificar : | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | Características del Inmueble : | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | | | | | | | | Propio | | | | | | | Rentado | | | | Prestado | | | | | | | | | | ||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | No. de Dormitorios | | | | | | No. de Baños | | | | Cocina | S i | | N o | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Servicio de Atención: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | Periodo del Año: | | | | | | | | | | | | | | | Días a la Semana: | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | Ciclo Escolar | | | | | | | | | | | | | | | | | L | M | M | J | V | S | D | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | Todo el Año | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | Horario: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Tipo de Población que Atiende: | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Sexo | | | | | | Masculino | | | | | | | Femenino | | | | | | Ambos | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | Tabla de Edades de Atención del Actor Social: | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | Población Objetivo | Número de Personas | Atención del Actor Social | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | Beneficiarias | Permanente 1/ | Interno 2/ | Externo 3/ | Eventual 4/ | Comunitario 5/ | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | Niñas y niños de 6 meses a 12 años de edad. | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | Mujeres y hombres adolescentes de 13 a 15 años. | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | Mujeres en periodo de gestación o lactancia. | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | Mujeres de 45 a 59 años. | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | Personas con enfermedades crónicas y personas con discapacidad. | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | Personas adultas de 60 y más años. | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | Total | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | 1/ Residen en las instalaciones. | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | 2/ Viven en las instalaciones, excepto los fines de semana o periodos vacacionales. | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | 3/ Permanecen sólo una parte del día en las instalaciones. | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | 4/ Su estancia en las instalaciones es irregular. | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | 5/ Personas atendidas en comunidad. | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| VI. CARACTERÍSTICAS GENERALES DE LAS PERSONAS ATENDIDAS |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Señale las principales características de las personas beneficiarias atendidas. | | | | | | | | | | | | | | | | ||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| VII. REQUISITOS SOLICITADOS PARA LA ATENCIÓN |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Edad : | | | | Si | | | No | | | | | | Cuota: | | | | Si | | | No | | | | | | | | | |||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | Promedio mensual por | | | | | | | | | | | | | | ||||||
| | | | | | | | | | | | | | | | | | Persona Beneficiaria : | $ | | | | | | | | | | | | | ||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Otros (Especifique): | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Observaciones: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| VIII. ALIMENTACIÓN QUE PROPORCIONA |
| | Servicio: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||
| | | Desayuno | Si | | No | | | | | Comida | Si | | No | | | Merienda | Si | | No | | | Cena | Si | | No | | ||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | ¿Es fijo el consumo de Leche? | | | | | | | | Si | | | No | | | | | | | | | | | | | | | | |||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | ¿Por qué? | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | Meses del año en los que varía la atención: | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | A) Disminuye | | | B) Aumenta | | ||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||
| | Frecuencia en el consumo de Alimentos: | | | Consumo de Leche de la Población Beneficiaria: | | | | | | | | | | | ||||||||||||||||||||||||||
| | Alimento | Número de días | | | Población Objetivo | No. de veces que toman leche al día | Litros de Leche | | | | ||||||||||||||||||||||||||||||
| | | | | | | a la semana | | | Diarios | Mensual | | | | |||||||||||||||||||||||||||
| | | Arroz | | | | | | | | | | Niñas y niños de 6 meses a 12 años de edad. | | | | | | | | | | | | | | | ||||||||||||||
| | | Carne * | | | | | | | | | | Mujeres y hombres adolescentes de 13 a 15 años. | | | | | | | | | | | | | | | ||||||||||||||
| | | Frijoles | | | | | | | | | | Mujeres en periodo de gestación o lactancia. | | | | | | | | | | | | | | | ||||||||||||||
| | | Fruta | | | | | | | | | Mujeres de 45 a 59 años. | | | | | | | | | | | | | | | |||||||||||||||
| | | Huevo | | | | | | | | | | Personas con enfermedades crónicas y personas con discapacidad. | | | | | | | | | | | | | | | ||||||||||||||
| | | Leche | | | | | | | | | | Personas adultas de 60 y más años. | | | | | | | | | | | | | | | ||||||||||||||
| | | Pan | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||
| | | Pescado | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||
| | | Sopa de Pasta | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||
| | | Tortilla | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||
| | | Verdura | | | | | | | | | ¿Reciben desayunos del DIF? | | | | Si | | No | | | | | | | | ||||||||||||||||
| | | Otros | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||
| | | (Especificar) | | | | | | | | Cantidad Mensual: | _____________________ | | | | | | | | | | | |||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | Leche equivalente a | ___________________ | | Litros/mes | | | | | | |||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | * Se contempla carne de Cerdo, Res y Pollo | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | ¿Atiende a personas u hogares que cuenten con Tarjeta de LICONSA? | | Si | | | No | | ¿Cuántas? | | | | | | | | |||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | ¿Están excluidas de la propuesta de posibles personas beneficiarias? | | Si | | | No | | | | | | | | | | | | | ||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| X. INGRESOS (Verificar con documentos) | ||||||||||||||||||||||||||||||||||||
| | ||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Origen | | | | | | | | | | | | | | | | | | | | | | Cantidad Mensual | | En Especie | | ||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | ( $ ) | | | | | | | | | ||
| | Subsidio | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Apoyos Privados | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Cuotas de Recuperación | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Otras fuentes de | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||
| | Ingresos (Especificar) | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Ingreso Promedio Mensual: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||
| | Observaciones: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||
| X. EGRESOS (Verificar con documentos) | | XI. OPINIÓN DEL RESPONSABLE DEL ESTUDIO | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Concepto | | Monto Mensual | | | El Actor Social visitado es candidato a la suscripción de Convenio | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | ( $ ) | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | Si | | | | | | | | No | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Agua | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Alimentos | | | | | | | | | | | ¿Por qué? | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Arrendamiento | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Luz | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Mantenimiento | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Predial | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Salarios | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Teléfono | | | | | | | | | | | | ¿Leche considerada a otorgar? | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Otros | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | Cantidad: | | | | | Litros | | Periodicidad: | | | | Mensual | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | Total | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | Cajas | | | | | | | | | Bimestral | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Observaciones Generales : | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | Persona del Actor social que proporcionó la Información | | | | | Persona de LICONSA que realizó el Estudio | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | (Bajo protesta de decir verdad) | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Nombre: | | | | | | | | | | | | | | | | | Nombre: | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Cargo: | | | | | | | | | | | | | | | | | Cargo: | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | Firma: | | | | | | | | | | | | | | | | | Firma: | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | Gerente del Centro de Trabajo | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | Sello del Actor Social | | | | | | | Nombre: | | | | | | | | | | | | | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | Firma: | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Anexo II
Lineamientos, Derechos y Obligaciones para el uso de la tarjeta de dotación de leche LICONSA
A) La tarjeta se otorga en beneficio de: niñas y niños de 6 meses a 12 años de edad; mujeres y hombres adolescentes de 13 a 15 años; mujeres en periodo de gestación o lactancia; mujeres de 45 a 59 años; personas con enfermedades crónicas o personas con discapacidad; personas adultas de 60 y más años.
B) La vigencia máxima de esta tarjeta es de un año, y deberá entregarse a la fecha de vencimiento al personal de promotoría social.
C) La venta de leche se realizará durante el horario establecido en el punto de venta.
D) Serán motivos de cancelación o retiro de la tarjeta:
a) Tener más de una tarjeta; haber proporcionado datos falsos; vender o hacer mal uso de la tarjeta.
b) Inasistencia continua de retiro de leche: 30 días en puntos de venta de leche líquida; 90 días en puntos de venta de leche en polvo.
c) Cometer faltas graves en el punto de venta como provocar desórdenes; alterar e impedir el suministro y venta de leche; hacer propaganda o proselitismo político o religioso.
E) LICONSA se reserva el derecho de abastecer leche en días festivos y periodos de contingencias.
Como persona beneficiaria de dotación de Leche LICONSA, tengo los siguientes:
| Derechos | Obligaciones |
| 1. Recibir un trato digno, respetuoso, oportuno, con calidad y equitativo, sin discriminación alguna. 2. Solicitar y recibir gratuitamente información acerca del Programa. 3. Adquirir la dotación de leche, en el horario y días establecidos en la tarjeta. 4. Tolerancia máxima de cinco minutos en el horario establecido, para la venta de leche líquida. 5. Recibir la dotación de leche sin condicionamiento a la compra de otros productos. 6. Obtener una nueva tarjeta por cambio de domicilio, extravío de la tarjeta o por registro de una nueva persona beneficiaria. 7. Presentar queja o denuncia ante LICONSA por irregularidades en el servicio. | 1. Tener sólo una tarjeta de dotación de leche, no transferirla, no venderla o hacer mal uso de ella. 2. Presentar la tarjeta en el horario establecido en la misma, y cuando el personal de LICONSA la solicite. 3. Acudir a los pases de lista y operativos de actualización y depuración del padrón de beneficiarios, previo aviso del personal de promotoría social. 4. Conservar en buen estado la tarjeta. |
Anexo III
Promotoría Social
El personal de promotoría social es la/el servidora (or) pública (o) de LICONSA que debe de cumplir con las siguientes funciones:
a) Recabar los datos socioeconómicos de los integrantes del hogar.
b) Actualizar y administrar el padrón de beneficiarios en los puntos de venta que se encuentran bajo su responsabilidad, conforme a la normatividad vigente.
c) Integrar, orientar y capacitar a los miembros del Comité de Beneficiarios, referente al buen funcionamiento de la operación del Programa.
d) Informar, orientar y capacitar a las/los concesionarias (os) y distribuidoras (res) mercantiles.
e) Vigilar el cumplimiento de los Lineamientos, Derechos y Obligaciones de las personas beneficiarias, que se encuentran impresos en la tarjeta de dotación de leche LICONSA.
f) Supervisar que la operación de los puntos de venta se realice dentro de los criterios normativos internos, así como realizar visitas domiciliarias.
g) Informar verbalmente a la persona solicitante de su aceptación o rechazo al programa.
El incumplimiento de las funciones antes referidas hará incurrir al personal de promotoría social en las sanciones previstas en la Ley Federal de Responsabilidades Administrativas de los Servidores Públicos y en la Ley General de Responsabilidades Administrativas.
Anexo IV
Convenio para el suministro de leche en polvo
Convenio para el suministro de leche en polvo que celebran por una parte LICONSA, Sociedad Anónima de Capital Variable, a la que en lo sucesivo se le denominará "LICONSA", representada en este acto por el (la) ----------------------------------, en su carácter de Apoderado(a), y por la otra parte ---------------------------------------------, a la que en lo sucesivo se le denominará el "Actor Social y Comunitario", representado por el (la) ------------------------------------, en su carácter de --------------------------, y a las que actuando de manera conjunta se les denominará "Las Partes", al tenor de las siguientes declaraciones y cláusulas.
D e c l a r a c i o n e s
1.- "LICONSA" declara a través de su representante:
1.1.- Que conforme a las leyes de los Estados Unidos Mexicanos, su representada se constituyó bajo la denominación de Rehidratadora de Leche Ceimsa, Sociedad de Participación Estatal Mayoritaria, creada mediante escritura pública número seis mil seiscientos sesenta y uno (6,661), de fecha dos de marzo de mil novecientos sesenta y uno, otorgada ante la fe del Licenciado Francisco Díaz Ballesteros, Notario Público número ciento veintinueve del Distrito Federal, e inscrita en el Registro Público de la Propiedad y del Comercio del Distrito Federal en el Libro tres, Volumen quinientos uno, a fojas ciento cincuenta y dos, bajo el número de partida ochenta y siete de la Sección de Comercio.
1.2.- Que su representada es una empresa de participación estatal mayoritaria de la Administración
Pública Federal, sectorizada en la Secretaría de Agricultura y Desarrollo Rural y después de diversas modificaciones a su denominación, actualmente ostenta la de "LICONSA", Sociedad Anónima de Capital Variable, según consta en la protocolización del acta de Asamblea General Extraordinaria de Accionistas celebrada el diecisiete de julio de mil novecientos noventa y cinco, otorgada en la escritura pública número veinticuatro mil novecientos setenta y uno (24,971) del quince de agosto de mil novecientos noventa y cinco, ante la fe del Licenciado Jesús Zamudio Villanueva, Notario Público número veinte del Municipio de Tlalnepantla, Estado de México, inscrita en el Registro Público de la Propiedad y del Comercio del Distrito Federal, con el folio mercantil número cuarenta y dos mil quinientos cincuenta y dos (42,552).
1.3.- Que el objeto social de su representada comprende, entre otras actividades, la de coadyuvar al fomento económico y social del país, participando en la adquisición y enajenación por cualquier título legal de leche fresca o en polvo, y de otros productos necesarios para su industrialización y la de sus derivados, en plantas propias o de terceros contratadas con los sectores público y privado, el procesamiento, distribución y de venta de leche fluida pasteurizada o en polvo y de otros productos lácteos y sus derivados, complementos alimenticios y otros productos derivados del aprovechamiento de sus procesos industriales, a los sectores urbanos y rurales en pobreza en establecimientos propios o de terceros, a través de cualquier canal de distribución que se precise en las Reglas de Operación del Programa de Abasto Social de Leche a cargo de la Entidad, la distribución y venta a precio preferencial de leche líquida, pasteurizada, rehidratada, ultrapasteurizada o en polvo, así como de complementos alimenticios, derivados lácteos u otros productos a través de cualquier canal de distribución y comercialización.
1.4.- Que el C. ----------------------- acredita su personalidad jurídica como Apoderado(a) de "LICONSA", mediante el testimonio de la escritura pública número ------------------------------------------ (-------), de fecha ------------- de ------------- de dos mil ------, otorgada ante la fe del Licenciado(a) -----------------, Notario Público número ------------ (-----), de ------------, manifestando que cuenta con facultades plenas para suscribir el presente convenio y que las mismas no le han sido limitadas, modificadas o revocadas en forma alguna.
1.5.- Que de conformidad con las Reglas de Operación del Programa de Abasto Social de Leche a cargo de "LICONSA", puede celebrar convenios con personas morales legalmente constituidas sin fines de lucro y con instituciones públicas de los tres órdenes de gobierno (federal, estatal y municipal), para suministrarle leche en polvo fortificada a precio subsidiado, al "Actor Social y Comunitario" que atiende a su población beneficiaria dentro y/o fuera de sus instalaciones.
1.6.- Que su Registro Federal de Contribuyentes es LIC-950821-M84.
1.7.- Que para los efectos de este convenio, su representada tiene establecido su domicilio en la Calle --------------- número -----------------------, Colonia -------------------------, Delegación Política, y/o Municipio ------------------, Código Postal --------------------- (--------).
2. El "Actor Social y Comunitario", declara a través de su representante:
2.1.- Que conforme a las leyes de los Estados Unidos Mexicanos, su representada está legalmente constituida como ------------------------------------, lo que acredita mediante el testimonio de la escritura pública número ---------------------------- (-------) de fecha --------- de -------- de dos mil ------, ante la fe del ----------------------------------, Notario Público número ------------------ (---), del --------------, inscrita en el Registro Público --------------------------- en la Sección de ---------------------- en ------------------------------------------------------.
2.2.- Que el (la) C. ------------------------------------------, acredita su personalidad jurídica como ---------------, mediante el testimonio de la escritura pública número ---------------- (----) de fecha ----------------------- de --------------------- de dos mil --------- otorgada ante la fe del Licenciado(a) ---------------------------------------, Notario Público número --------------- (----), de ---------, inscrita en el Registro Público --------------------------- en la Sección de ---------------------- en -----------------------------------------------; y quien se identifica con la credencial para votar, vigente, con el folio número -------------------, y número identificador (OCR) -------------------, expedida a su favor por el Instituto Nacional (Federal) Electoral, manifestando que cuenta con facultades plenas para suscribir el presente convenio y que las mismas no le han sido limitadas, modificadas o revocadas en forma alguna.
2.3.- Que entre los objetivos de su representada se encuentra principalmente el de --------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------.
2.4.- Que de conformidad con su objeto social, solicita a "LICONSA" la celebración del presente convenio, a efecto de que le sea suministrada leche en polvo fortificada a precio subsidiado, para la población que atiende, la cual cumple con los requisitos establecidos en las Reglas de Operación del Programa de Abasto Social de Leche a cargo de "LICONSA", para ser considerada persona beneficiaria de "LICONSA".
2.5.- Que su Registro Federal de Contribuyentes es ------------------.
2.6.- Que su Clave Única de Inscripción al Registro Federal de las Organizaciones de la Sociedad Civil (CLUNI) es -----------------------.
2.7.- Que para el ejercicio de sus derechos y cumplimiento de sus obligaciones de este convenio, su representada tiene establecido su domicilio fiscal en la Calle ---------------------------------------------- número ----------------------, Colonia --------------------------, Delegación Política, y/o Municipio --------------------------, Código Postal ------------------------ (--------).
3.- "Las Partes" declaran:
3.1.- Que se reconocen mutuamente la personalidad jurídica con que acuden a la celebración del presente convenio.
3.2.- Que en virtud de las declaraciones señaladas, es su voluntad celebrar el presente convenio, obligándose recíprocamente en sus términos y someterse a lo dispuesto en los diversos ordenamientos encargados de regular los actos jurídicos de esta naturaleza.
Una vez reconocida plenamente la personalidad y capacidad jurídica con que comparecen, es su voluntad celebrar el presente acto jurídico, para lo cual están de acuerdo en sujetarse a las siguientes:
C l á u s u l a s
Primera.- Objeto
El presente convenio tiene como propósito establecer el suministro de leche en polvo fortificada a precio subsidiado de "LICONSA", (en lo sucesivo la "Leche") al "Actor Social y Comunitario", para que se destine únicamente a complementar la alimentación y nutrición de la población que atiende, conformada por hasta ------------- (-------) personas beneficiarias constituidas por (describir el tipo de población objetivo que se va a atender), quienes son atendidas en las unidades operativas indicadas en el Anexo I, que firmado por "Las Partes" forma parte integrante del presente instrumento.
El apoyo alimentario a las personas beneficiarias se dará hasta ------------------------- (-------) días al mes, y el "Actor Social y Comunitario" se compromete a que cada una de ellas consuma hasta ---------------- (-------) mililitros de la "Leche" al día. De acuerdo al Tipo y Monto de Apoyo establecido en las Reglas de Operación vigentes para cada persona beneficiaria.
Segunda.- Personas beneficiarias y Requerimientos de la "Leche"
El "Actor Social y Comunitario" se compromete a proporcionar a "LICONSA" durante los tres (3) primeros días naturales de cada entrega calendarizada, el padrón de personas beneficiarias atendidas en el periodo anterior, como se indica en el Anexo II, que firmado por "Las Partes" se integra al presente instrumento, el cual estará conformado por los siguientes datos:
1) Nombre completo de las personas beneficiarias (apellido paterno, materno, nombre(s).
2) Fecha de nacimiento.
3) Sexo
4) Estado de Nacimiento
5) Edad.
6) Clave Única de Registro de Población (CURP).
7) Estado Civil
8) Domicilio de la persona beneficiaria.
Así mismo, el "Actor Social y Comunitario" deberá entregar, bajo protesta de decir verdad, el padrón nominal antes mencionado manifestando expresamente que las personas beneficiadas por su conducto no reciben el apoyo de "Leche" por el esquema de abasto comunitario.
Con dicha información "LICONSA" puede constatar que los destinatarios de la "Leche" corresponden a su población objetivo, sin perjuicio de que cualquier desviación a la misma, "LICONSA" podrá reclamar los daños y perjuicios que ésta le genere.
El "Actor Social y Comunitario" realizará por escrito a "LICONSA", el requerimiento de la "Leche" durante los primeros tres (3) días del periodo inmediato anterior, especificando el número de personas beneficiarias a atender, así como el número de litros requeridos en cajas cerradas con treinta y seis (36) sobres de --------------------- (------) gramos cada uno, equivalentes a dos (2) litros de la "Leche".
Tercera.- Ampliación de Operaciones
Para el caso de que el "Actor Social y Comunitario" requiera aumentar el número de personas beneficiarias a atender, presentará a "LICONSA" solicitud por escrito con al menos treinta (30) días naturales de anticipación, indicando el número de personas beneficiarias adicionales a atender, así como la cantidad de la "Leche" requerida, manifestando que corresponden a personas que por sus características se encuentran dentro de la población objetivo de "LICONSA".
Por su parte, "LICONSA" dará respuesta oportuna al "Actor Social y Comunitario" una vez evaluada su viabilidad, a efecto de determinar la posibilidad de aumentar el suministro de la "Leche" y la incorporación de las personas beneficiarias.
Una vez aprobada por "LICONSA" la ampliación del número de personas beneficiarias, se procederá a la formalización de un convenio modificatorio.
Cuarta.- Precio de la "Leche"
El precio por cada litro de la "Leche", que "LICONSA" suministre al "Actor Social y Comunitario", en términos del presente convenio, será de $ ------- (----------------------- pesos ----/100 M.N), por lo que será un precio de $ ------------ (-------------------- pesos ----/100 M.N) por cada sobre de ----------------- gramos, equivalente a dos (2) litros de la "Leche". Este precio será modificado cuando el Consejo de Administración de "LICONSA" así lo determine, debiendo notificarlo por escrito al "Actor Social y Comunitario", a efecto de que proceda su aplicación en el surtimiento posterior, inmediato, sin que exista formalidad adicional alguna.
Por su parte, el "Actor Social y Comunitario" podrá dar en venta únicamente a las personas beneficiarias consideradas en este instrumento, la "Leche" que "LICONSA" le suministre, sin incrementar el precio por litro autorizado por "LICONSA".
Quinta.- Forma de Pago
El "Actor Social y Comunitario" realizará el pago de la "Leche" solicitada, previo a la entrega de la misma, mediante depósito en efectivo en caja, o cheque certificado a nombre de Liconsa, S.A. de C.V., en las oficinas de -----------------------------------------.
Asimismo, podrá pagar con 5 días hábiles previos a la entrega de la "Leche", a través de transferencia electrónica (sistema SIAF) a la cuenta bancaria número ---------------- sucursal ----, plaza -------------, clabe de transferencia interbancaria --------------- del Banco ----------- a nombre de LICONSA, Sociedad Anónima de Capital Variable; proporcionando "LICONSA" la factura correspondiente.
"Las Partes" acuerdan que en el caso de que no se cumpla con el pago anticipado, no se efectuará el surtimiento de la "Leche" requerida, sin que se incurra en responsabilidad alguna por "LICONSA".
Sexta.- Entrega - Recepción de la "Leche"
El "Actor Social y Comunitario" autorizará por escrito al personal responsable de esa Institución, quien previa identificación, recibirá la "Leche" en el almacén general de --------------------------------------------------, ubicado en la Calle ----------------------------- número -------------- (----) Colonia -----------------------------, Municipio -----------------, Código Postal --------------- (-----).
La entrega-recepción de la "Leche" podrá efectuarse en los días y horarios que acuerden "Las Partes". En cada entrega, el personal autorizado por el "Actor Social" deberá firmar de recibido en la(s) factura(s) que el personal de "LICONSA" le entregue.
Séptima.- Manejo y Conservación de la "Leche"
Una vez que "LICONSA" entregue la "Leche" al "Actor Social y Comunitario", éste se compromete a tomar en todo momento, las medidas necesarias y suficientes para el debido manejo y conservación de la misma, a efecto de que no caduque, ni pierda sus cualidades sanitarias y nutricionales; no podrá realizar acciones proselitistas, asumiendo totalmente la responsabilidad de su utilización, control y destino.
El "Actor Social y Comunitario" se compromete a no comercializar la "Leche" con personas distintas a las indicadas en la cláusula primera de este instrumento; a no desviarla para fines distintos a los acordados; o bien a alterar el contenido de los sobres.
"LICONSA" se obliga a que la "Leche", se encuentre en las mejores condiciones de integración, sanidad y manejo, cumpliendo la Norma Oficial Mexicana NOM-243-SSA1-2010, publicada en el Diario Oficial de la Federación el veintisiete (27) de septiembre de dos mil diez.
Octava.- Supervisión
El "Actor Social y Comunitario" se compromete a brindar las facilidades que sean necesarias a "LICONSA" a fin de que pueda llevar a cabo la supervisión que permita verificar el almacenamiento, preparación, suministro, manejo, y en su caso el destino de la "Leche".
"Las Partes" se comprometen a celebrar reuniones cuando así lo solicite alguna de éstas con la finalidad de resolver cualquier problema de carácter operativo que se presente.
Novena.- Evaluaciones
El "Actor Social" presentará periódicamente a "LICONSA", información relativa a las evaluaciones, muestreos o seguimientos que, en su caso, realice sobre los beneficios del consumo de "Leche" entre la población atendida, clasificada por rangos de edad y género.
Décima.- Cesión de Derechos
Los derechos y obligaciones del presente convenio, no podrán ser cedidos, vendidos, traspasados, enajenados o donados a terceros. Salvo a solicitud expresa y por escrito del "Actor Social y Comunitario", para lo cual se formalizará un convenio modificatorio al presente.
Décima Primera.- Vigencia y Terminación
El presente convenio se celebra por tiempo indefinido, siempre y cuando prevalezcan las condiciones normativas y presupuestales que así lo permitan, iniciando su vigencia a partir del día ----------------------, asimismo podrán darlo por terminado anticipadamente cualquiera de "Las Partes", sin incurrir en responsabilidad alguna, previo aviso por escrito con al menos treinta (30) días naturales de anticipación, previo cumplimiento de las obligaciones contraídas.
Décima Segunda.- Rescisión
En caso de incumplimiento de las obligaciones contraídas por el "Actor Social y Comunitario" en el presente convenio, procederá la rescisión del mismo sin ninguna responsabilidad para "LICONSA" y sin necesidad de promover acción judicial; en el caso de que la "Leche" o el precio sean alterados por el "Actor Social y Comunitario" este será el único responsable de los daños o perjuicios que cause tal hecho, debiendo responder directamente o bien resarcir a "LICONSA" los gastos que tenga que erogar por tales conceptos.
"LICONSA", podrá ejecutar las acciones legales procedentes en el caso de que exista algún perjuicio o
daño.
Décima Tercera.- Modificaciones
El presente convenio podrá ser adicionado o modificado a petición expresa y por escrito de cualquiera de "Las Partes", una vez acordados los términos y condiciones a modificar, quedarán plasmadas en el convenio modificatorio correspondiente, las cuales entrarán en vigor a la fecha de su firma.
Décima cuarta.- Relación Laboral
"Las Partes" manifiestan expresamente que para el objeto del cumplimiento del presente convenio, requieren hacer uso de su personal, reconociendo que cada parte, será la única responsable de las relaciones laborales con sus trabajadores, al contar con elementos propios suficientes para responder ante ellos de sus obligaciones laborales, por lo que cada una de las partes, en ningún momento será considerada como intermediaria ni tendrá ninguna responsabilidad de la relación laboral respecto a los trabajadores de la otra, por lo que éstas se obligan a responder por cualquier conflicto laboral que surja con sus trabajadores, relevando a la otra parte de cualquier responsabilidad y comprometiéndose por lo tanto a sacarla a salvo y en paz de cualquier conflicto laboral, así como de la responsabilidad ante terceros y asumirán sus responsabilidades fiscales y de seguridad social y en ningún caso serán consideradas como patrones solidarios o substitutos.
Décima Quinta- Legislación Aplicable
"Las Partes" convienen en que para todo lo no previsto en el presente convenio, se estará a lo dispuesto en la Ley Orgánica de la Administración Pública Federal, la Ley Federal de las Entidades Paraestatales, la Ley de Planeación, las Reglas de Operación del Programa de Abasto Social de Leche a cargo de "LICONSA", el Manual de Procedimientos para la Operación de los Convenios con Actores Sociales y en su caso, el Código de Comercio y Código Civil Federal, así como en lo dispuesto en las demás disposiciones legales aplicables.
Décima Sexta.- Jurisdicción
Cualquier controversia con respecto a la interpretación y cumplimiento de este convenio, será resuelta entre "Las Partes", dentro de un plazo de quince (15) días naturales contados a partir de que alguna de ellas manifieste por escrito a la otra, el punto de controversia o incumplimiento. Sólo en caso de no llegar a ningún acuerdo o solución se someterán a la jurisdicción de los Tribunales Federales con residencia en ---------- (ajusta al lugar de operación) ---------------, renunciando a cualquier otro fuero que pudiera corresponderles con motivo de sus domicilios presentes o futuros.
Enteradas "Las Partes" del alcance, contenido y fuerza legal del presente convenio, y por no mediar vicio alguno del consentimiento, ni contener cláusula contraria a derecho, lo firman al margen y al calce por cuadruplicado de conformidad los que en el presente instrumento intervienen, en unión de los testigos que de igual manera lo hacen en la Ciudad de ---------------- a; -------------------------------------.
| Por "LICONSA" -------------------------- (Nombre, Cargo y Firma) | Por "Actor Social y Comunitario" -------------------------- (Nombre, Cargo y Firma) |
T e s t i g o s
| -------------------------- (Nombre, Cargo y Firma) | -------------------------- (Nombre, Cargo y Firma) |
Revisión Legal
_____________________________
Dirección de Asuntos Jurídicos
Anexo IV.1
Actor Social y Comunitario:
| Número | Nombre de la Unidad Operativa |
| | |
| | |
| | |
| | |
| | |
Anexo IV.2
Padrón Nominal de Personas Beneficiarias
Nombre de la Unidad Operativa:
| No. 1/ | Apellido Paterno 2/ | Apellido Materno 3/ | Nombre (s) 4/ | Fecha de Nacimiento 5/ | Sexo 6/ | Entidad Federativa de Nacimiento 7/ | Edad 8/ | CURP 9/ | Estado Civil 10/ | Domicilio de la Unidad Operativa 11/ |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
1/ Número consecutivo.
2/Primer Apellido de la persona beneficiaria.
3/ Segundo Apellido de la persona beneficiaria.
4/ Nombre(s) de la persona beneficiaria.
5/ Fecha de nacimiento de la persona beneficiaria. (aaaa/mm/dd)
6/ Clave del sexo de la persona beneficiaria, donde: H = Hombre y M = Mujer.
7/ Clave de la Entidad Federativa de nacimiento de la persona beneficiaria.
8/ Años cumplidos de la persona beneficiaria. (dos enteros con un decimal)
9/ Clave Única de Registro de Población de la persona beneficiaria.
10/ Clave del estado civil de la persona beneficiaria.
11/ Domicilio de la unidad operativa. (lugar donde recibe el beneficio)
Anexo V
Convenio modificatorio al convenio para el suministro de leche en polvo
Convenio modificatorio al convenio para el suministro de leche en polvo, con número de registro ___________________, en lo sucesivo "El Convenio Principal", que celebran por una parte LICONSA, Sociedad Anónima de Capital Variable, a la que en lo sucesivo se le denominará "LICONSA", representada en este acto por el (la) __________________, en su carácter de Apoderado(a), y por la otra parte ____________________ , a la que en lo sucesivo se le denominará el "Actor Social y Comunitario", representado por el (la) _________________________, en su carácter de __________________ , y que actuando de manera conjunta se les denominará "Las Partes", al tenor de las siguientes declaraciones y cláusulas.
D e c l a r a c i o n e s
1. Declara el representante de "LICONSA":
1.1 Que acredita su personalidad jurídica como Apoderado(a) de "LICONSA", mediante el testimonio de la Escritura Pública número __________________________________, de fecha _______________________, otorgada ante la fe del Licenciado(a) ________________, Notario Público número ______________, de __________________. Manifestando que las facultades ahí otorgadas, no le han sido limitadas, modificadas o revocadas en forma alguna.
2. Declara el representante del "Actor Social y Comunitario":
2.1 Que acredita su personalidad jurídica como ______________ del "Actor Social y Comunitario", mediante el testimonio de la Escritura Pública número ______________________, de fecha _____________, otorgada ante la fe del _______________________, Notario Público número ______________, del _______________. Manifestando que las facultades ahí otorgadas, no le han sido limitadas, modificadas o revocadas en forma alguna.
3. Declaran "Las Partes":
3.1 Que con fecha ________________, sus representadas celebraron "El Convenio Principal", con el propósito de unir sus recursos y esfuerzos para llevar a cabo la distribución y dotación mensual de leche en polvo a precio subsidiado para apoyar la alimentación de _________________ que reciben atención por medio del "Actor Social y Comunitario". Mismo que fue inscrito en el Registro Consecutivo Nacional el día __________________, con el número _______________.
3.2 Que en la cláusula Primera.- Objeto, de "El Convenio Principal" se estableció:
Primera.- Objeto
El presente convenio tiene como propósito establecer el suministro de leche en polvo fortificada a precio subsidiado de "LICONSA", (en lo sucesivo la "Leche") al "Actor Social y Comunitario", para que se destine únicamente a complementar la alimentación y nutrición de la población que atiende, conformada por hasta _________________ (____) personas beneficiarias, quienes son atendidas en las unidades operativas indicadas en el Anexo I, que firmado por "Las Partes" forma parte integrante del presente instrumento.
El apoyo alimentario a las personas beneficiarias se dará hasta ____________ (____) días al mes, y el
"Actor Social y Comunitario" se compromete a que cada una de ellas consuma hasta _________ (_____) mililitros de la "Leche" al día. De acuerdo al Tipo y Monto de Apoyo establecido en las Reglas de Operación vigentes para cada persona beneficiaria.
3.3 Que en virtud de las anteriores declaraciones, es voluntad e interés de "Las Partes", modificar _______________________________, mediante la celebración del presente instrumento, permaneciendo en vigor las restantes cláusulas del "Convenio Principal" siempre y cuando no contravengan a los términos de lo pactado en el presente Convenio Modificatorio.
Vistas las anteriores declaraciones "Las Partes" se obligan al tenor de las siguientes:
C L Á U S U L A S
Primera.- Objeto Modificar ___________________. (Establecer el caso en particular de la parte que se modifica), para quedar de la siguiente manera:
Redactar textualmente lo que se va a modificar.
Ejemplo: Si el caso fuera dotación, o personas beneficiarias sería la cláusula primera, y si aplica el caso, la modificación en los Anexos respectivos.
El presente convenio tiene como propósito establecer el suministro de leche en polvo fortificada a precio subsidiado de "LICONSA", (en lo sucesivo la "Leche") al "Actor Social y Comunitario", para que se destine únicamente a complementar la alimentación y nutrición de la población que atiende, conformada por hasta ------------------ (-------) personas beneficiarias constituidas por (describir el tipo de población objetivo que se va a atender), quienes son atendidas en las unidades operativas indicadas en el Anexo I, que firmado por "Las Partes" forma parte integrante del presente instrumento.
El apoyo alimentario a las personas beneficiarias se dará hasta __________________ (____) días al mes, y el "Actor Social y Comunitario" se compromete a que cada una de ellas consuma hasta ____________ (_____) mililitros de la "Leche" al día. De acuerdo al Tipo y Monto de Apoyo establecido en las Reglas de Operación vigentes para cada persona beneficiaria.
Segunda.- Validez
"Las Partes" acuerdan que el demás clausulado del convenio referido en el apartado 3.1 anterior, se mantendrá vigente en lo que no se contravenga a los términos planteados en el presente instrumento, y éste tendrá validez a partir del día de su suscripción.
Enteradas "Las Partes" del alcance, contenido y fuerza legal del presente convenio y por no contener dolo, error, mala fe, ni ningún vicio de voluntad ni cláusula contraria a derecho, y para los efectos legales a que haya lugar lo firman de común acuerdo, por cuadruplicado, al margen y al calce los que en este instrumento intervienen ante la presencia de los testigos que de igual manera lo hacen, en la ciudad de ___________ el día ____________________________.
| Por "LICONSA" ------------------------------------ (Nombre, Cargo y Firma) | Por el "Actor Social y Comunitario" ------------------------------------ (Nombre, Cargo y Firma) |
T e s t i g o s
| ---------------------------------- (Nombre, Cargo y Firma) | ---------------------------------- (Nombre, Cargo y Firma) |
Revisión Legal
_____________________________
Dirección de Asuntos Jurídicos
Anexo VI
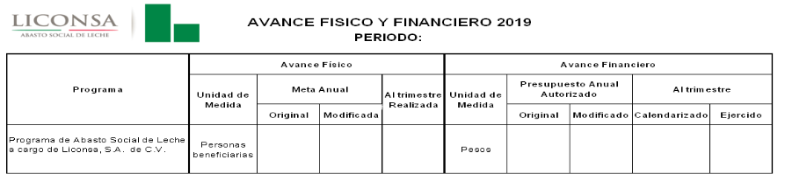
Anexo VII
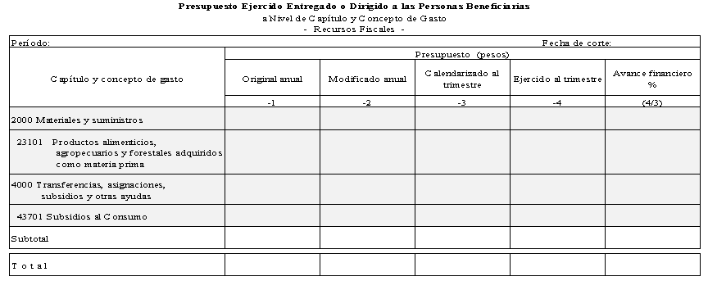
Anexo VIII
Indicadores de reglas de operación 2020 del Programa de Abasto Social de Leche
| Nombre | Fórmula | Unidad de Medida | Frecuencia de Medición |
PROPÓSITO
| Margen de ahorro por litro de leche de las familias beneficiarias del programa | [(Precio comercial de leches equivalentes a la leche distribuida por LICONSA menos precio de leche LICONSA) entre precio comercial de leches equivalentes a la leche distribuida por LICONSA] por 100 | Porcentaje | Trimestral |
| Porcentaje de cobertura de los hogares potenciales | (Hogares atendidos entre Hogares potenciales de la Nota de Población Potencial y Población objetivo del PASL) por 100 | Porcentaje | Trimestral |
COMPONENTE
| Promedio de litros distribuidos por beneficiario al mes ( Factor de retiro) | Litros distribuidos entre número de beneficiarios | Litros | Trimestral |
| Porcentaje de mujeres atendidas por el PASL, respecto al total de beneficiarios | (Total de población femenina atendida entre Total de población beneficiaria) por cien | Porcentaje | Trimestral |
| Porcentaje de beneficiarios niñas y niños menores de 5 años respecto del total del padrón | (Niñas y niños menores de 5 años atendidos entre Total de población beneficiaria) por cien | Porcentaje | Trimestral |
| Porcentaje de beneficiarios por niñas y niños de 6 meses a 12 años de edad respecto del total del padrón | (Niñas y niños de 6 meses a 12 años atendidos entre Total de población beneficiaria) por cien | Porcentaje | Trimestral |
| Porcentaje de mujeres y hombres adolescentes de 13 a 15 años beneficiarias respecto del total del padrón | (Mujeres y hombres adolescentes de 13 a 15 años atendidas entre Total de población beneficiaria) por cien | Porcentaje | Trimestral |
| Porcentaje de mujeres de 45 a 59 años beneficiarias respecto del total del padrón | (Mujeres de 45 a 59 años atendidas entre Total de población beneficiaria) por cien | Porcentaje | Trimestral |
| Porcentaje de mujeres en período de gestación o lactancia beneficiarias respecto del total del padrón | (Mujeres en período de gestación o lactancia atendidas entre Total de población beneficiaria) por cien | Porcentaje | Trimestral |
| Porcentaje de enfermos crónicos y personas con discapacidad beneficiarias respecto del total del padrón | (Enfermos crónicos y personas con discapacidad atendidas entre Total de población beneficiaria) por cien | Porcentaje | Trimestral |
| Porcentaje de adultos mayores de 60 y más años beneficiados respecto del total del padrón | (Adultos mayores de 60 y más años atendidos entre Total de población beneficiaria) por cien | Porcentaje | Trimestral |
| Porcentaje de cumplimiento de atención a la población objetivo | (Población atendida entre Población objetivo) por cien | Porcentaje | Trimestral |
| Porcentaje de cumplimiento del Programa de Distribución | (Litros distribuidos entre Litros programados) por cien | Porcentaje | Trimestral |
Anexo IX
Esquema de Contraloría Social
I. Difusión
Los procedimientos para realizar las tareas de Contraloría Social se difundirán por medio de carteles informativos. La Unidad de Comunicación Social será la encargada de su elaboración bajo la supervisión de la Dirección de Abasto Social.
Los carteles se distribuirán a los Centros de Trabajo a fin de que se coloquen en los puntos de venta.
Las personas responsables de verificar que el material se encuentre ubicado de manera adecuada es el personal de promotoría social.
Otro medio de difusión es mediante la página web www.gob.mx/liconsa, en la que se puede consultar el Programa de Abasto Social de Leche (PASL).
II. Capacitación y asesoría
El personal del Departamento de Seguimiento Operativo será el responsable de capacitar a las/los servidoras(es) públicas(os), que asignen los Centros de Trabajo.
Las/los representantes de las actividades de Contraloría Social en los Centros de Trabajo capacitarán al personal de promotoría social.
El personal de promotoría social son las/los servidoras(es) públicas(os) responsables de llevar a cabo la constitución y renovación de los comités de beneficiarios, de brindarles la capacitación y asesoría necesaria, así como de captar los informes emitidos por los comités.
El personal de promotoría social deberá considerar que en la conformación de los comités exista la paridad entre mujeres y hombres.
III. Seguimiento
Para monitorear el cumplimiento de las actividades de promoción de Contraloría Social se utilizarán los siguientes instrumentos:
· Informes Bimestrales del avance del registro de información del Sistema Informático de Contraloría Social (SICS) de la Secretaría de la Función Pública.
· Informes de los Comités que describen las actividades y los resultados de Contraloría Social en los puntos de venta.
Es compromiso de los integrantes de los Comités, el llenado de los informes, con el propósito de registrar las actividades de seguimiento, supervisión y vigilancia.
IV. Actividades de Coordinación
Los Centros de Trabajo de LICONSA son los encargados de la correcta vigilancia y seguimiento de las acciones de Contraloría Social.
La Cláusula de Contraloría Social para convenios de Coordinación no aplica para el Programa.
Anexo X. Información Socioeconómica
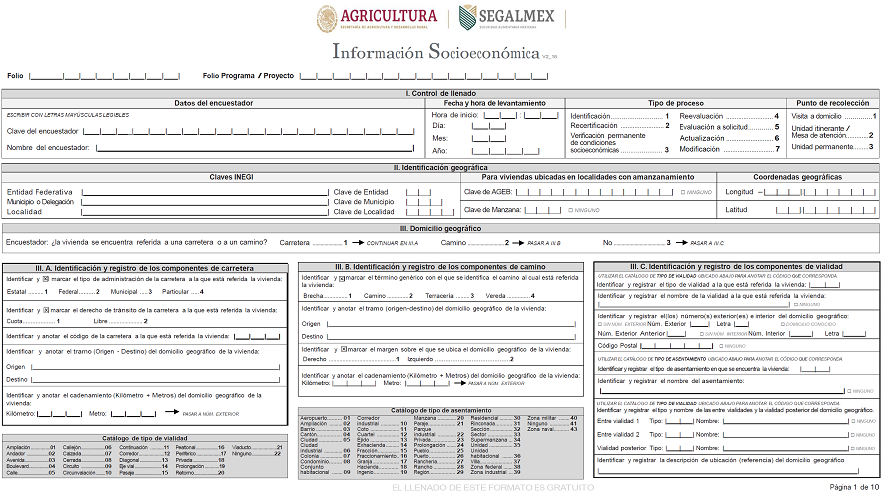
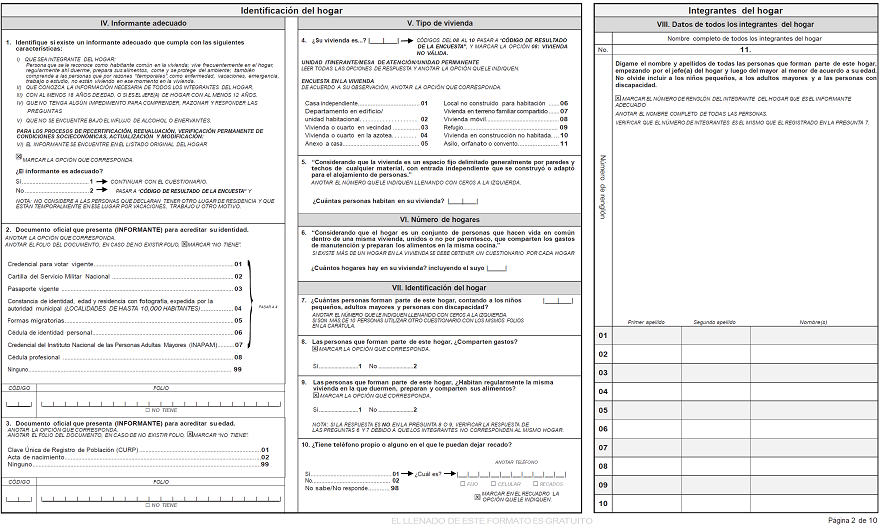
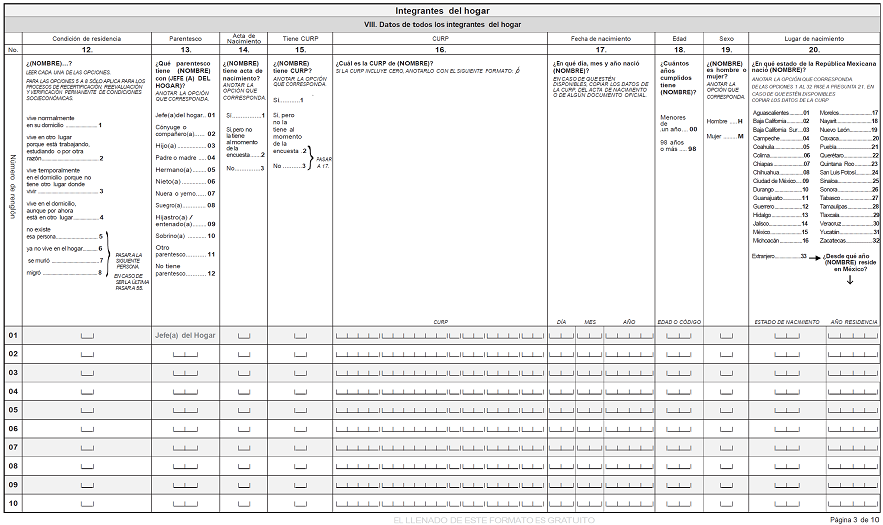
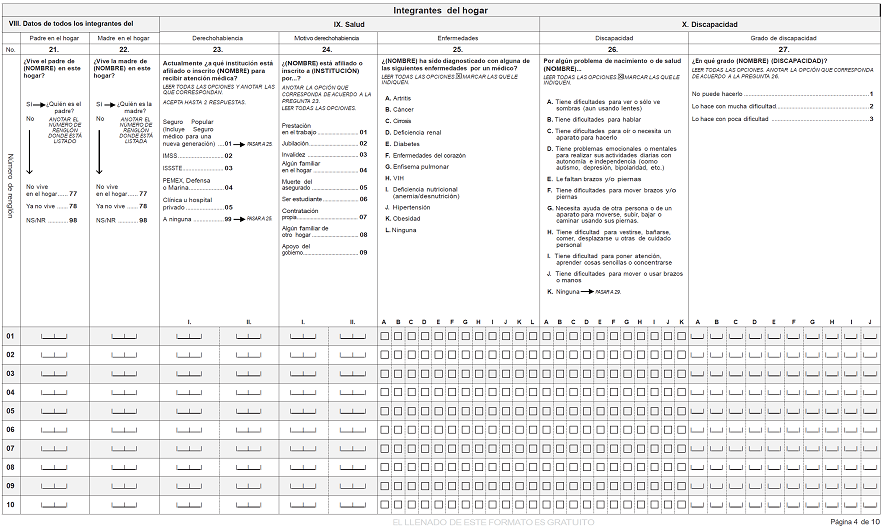
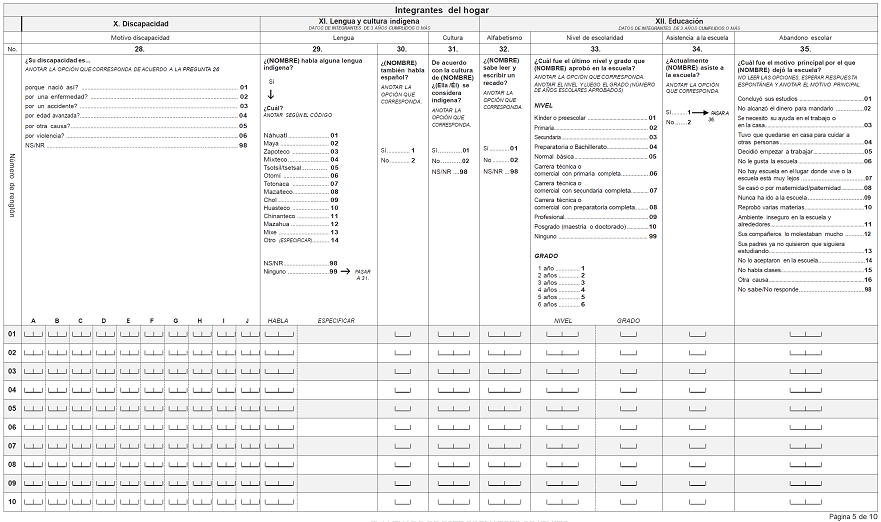
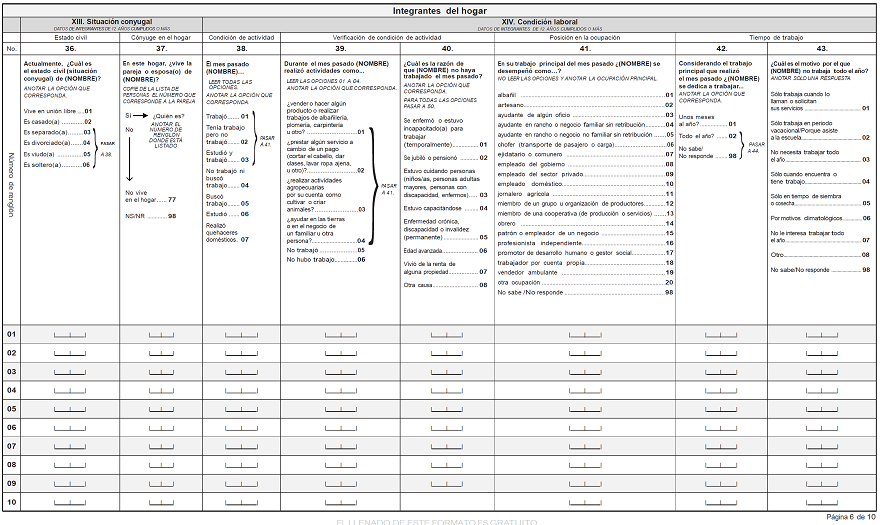
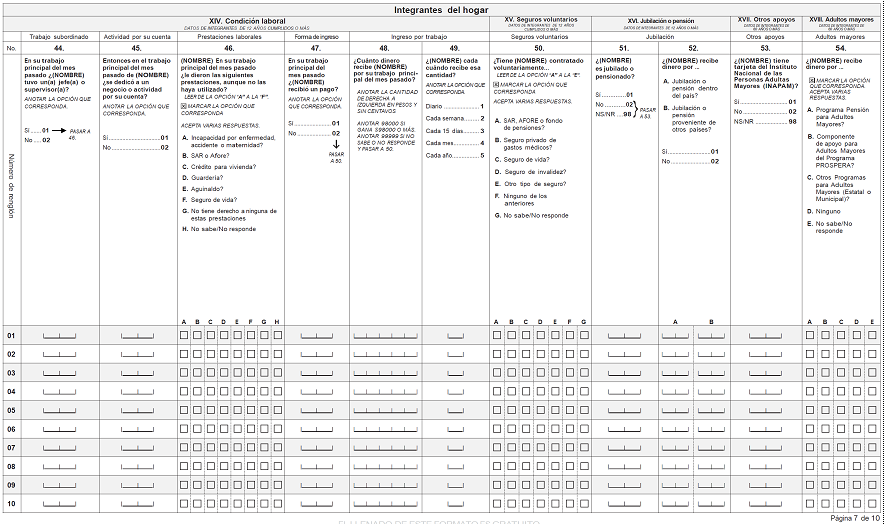
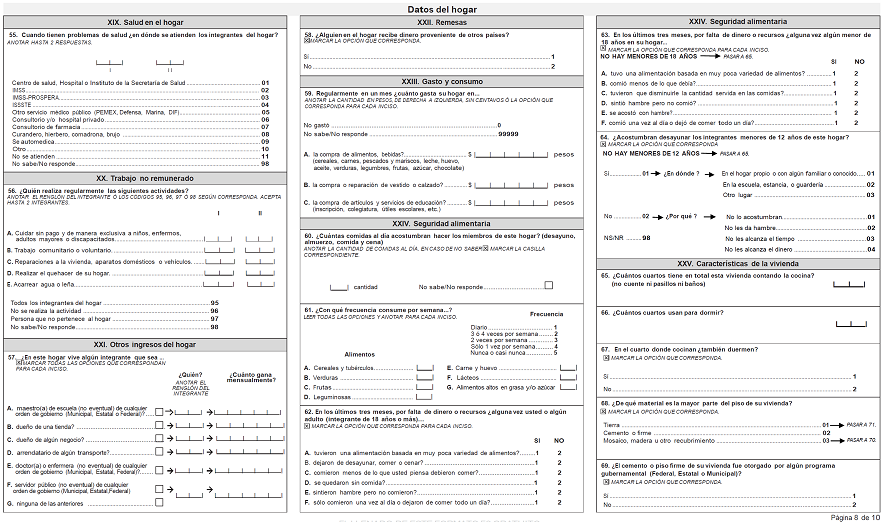
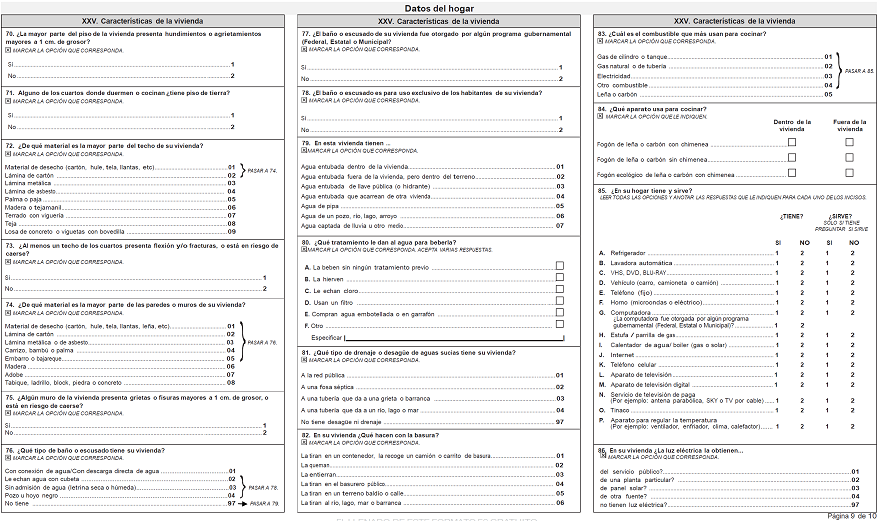
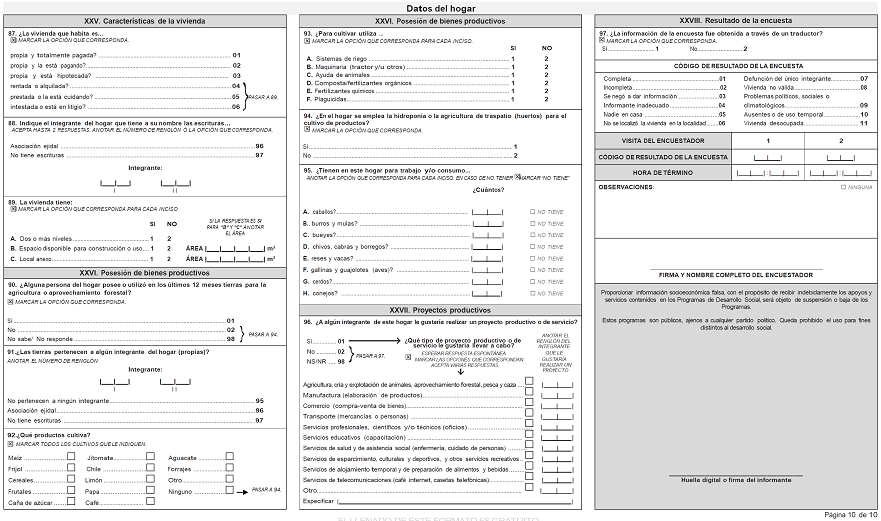
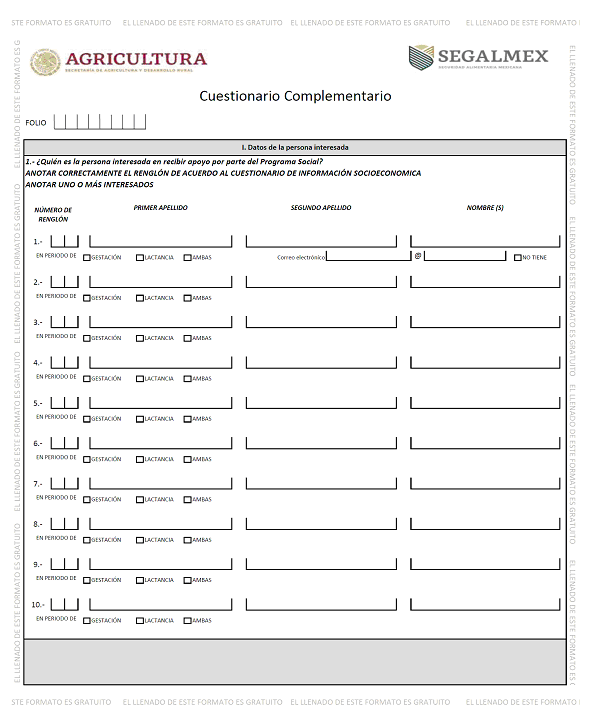
Anexo XI. Cuestionario Único de Actores Sociales
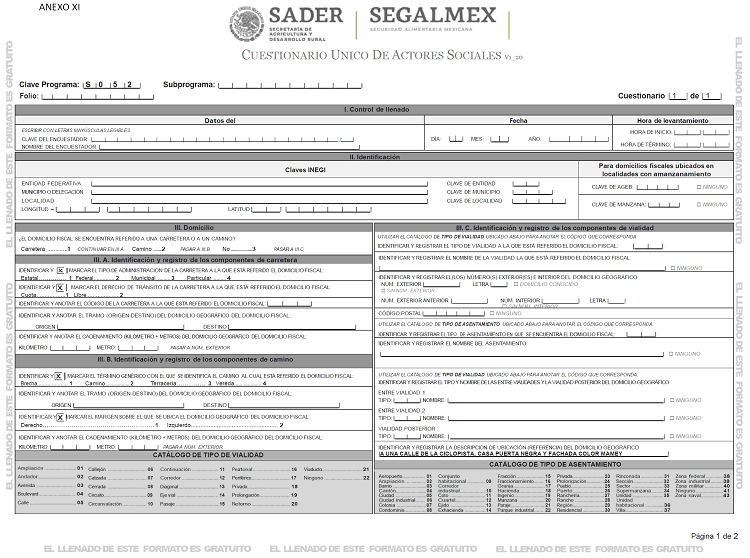
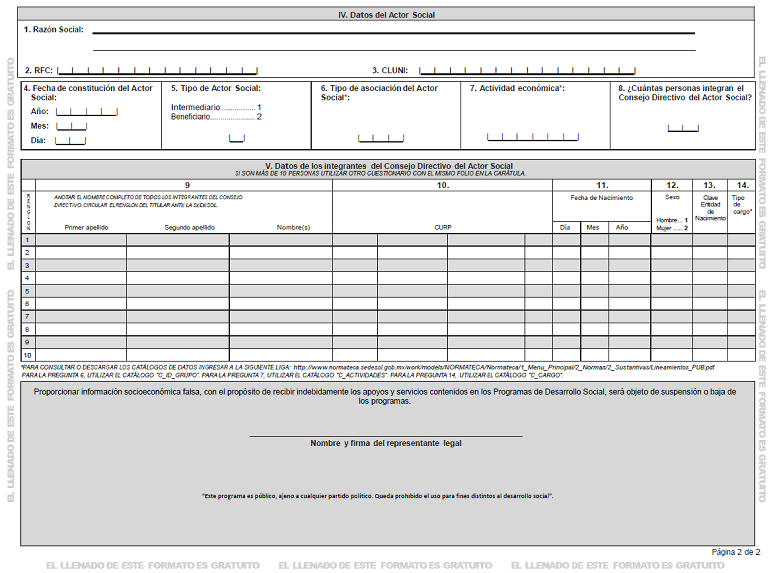
Anexo XII. Flujograma para Solicitar la Incorporación al Padrón de Beneficiarios
OBJETIVO: Contribuir al bienestar social e igualdad mediante el mejoramiento en el acceso a la alimentación de las personas integrantes de los hogares beneficiarios.
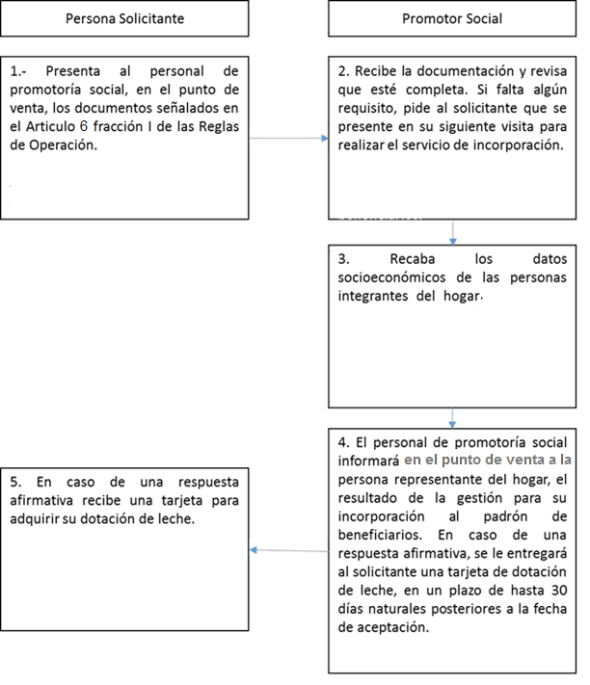
Anexo XIII.- Flujograma para Solicitar Nuevos Puntos de Venta
OBJETIVO: Contribuir al bienestar social e igualdad mediante el mejoramiento en el acceso a la alimentación de las personas integrantes de los hogares beneficiarios.
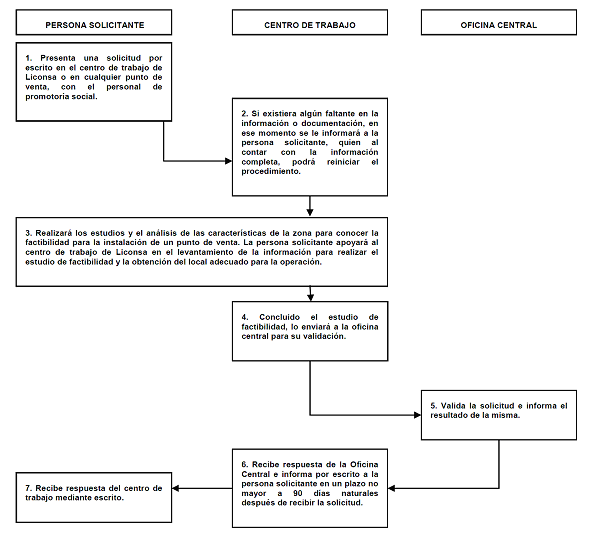
Anexo XIV. Flujograma Convenios con Actores Sociales y Comunitarios
OBJETIVO: Contribuir al bienestar social e igualdad mediante el mejoramiento en el acceso a la alimentación de las personas beneficiarias, atendidas a través de los Actores Sociales y Comunitarios.
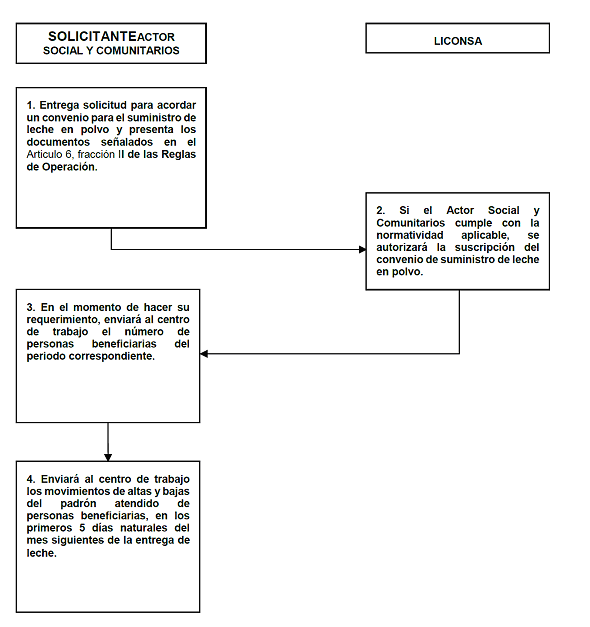
Anexo XV. Flujograma Convenio Modificatorio con Actores Sociales y Comunitarios
OBJETIVO: Contribuir al bienestar social e igualdad mediante el mejoramiento en el acceso a la alimentación de las personas beneficiarias, atendidas a través de los Actores Sociales y Comunitarios.
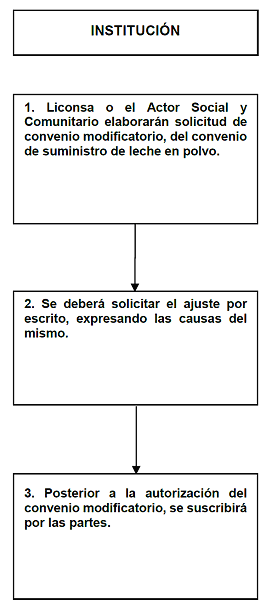
______________________________